(ITUNES OR Listen Here)
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The overarching theme to Day 1 at SMACC? Use your team- to keep you in check and for feedback. Our cases and errors are opportunities for reflection. Dr. Cliff Reid reminded us to follow up our patients and outcomes and learn from it all, without letting our egos get in the way. Dr. Simon Carley (St. Emlyn’s) gave a powerful talk on learning from mistakes later in the day; you will definitely want to listen to these when they come out.
The sub theme? Experts don’t need algorithms and tests. But the novices? That’s another story.
Trauma – Weingart. We won’t delve into his thoughts on ATLS here (hint: ATLS isn’t for experts).
- Ignore the first automated blood pressure, it’s probably wrong. Get a manual blood pressure.
- Giving 3 units of blood in one hour? Prepare for massive transfusion, that means FFP, platelets, everything
- If you go down the massive transfusion pathways, give an ampule of calcium every 4-6 units of plasma to combat the transfusion induced hypocalcemia from citrate.
- The Shock Index (HR/SBP), isn’t as exciting as we once thought. It may be a guide, but not reliably so.
Pain – Strayer
- Analgesia doesn’t = opiates. Think about local analgesia.
- Pain as the “5th vital sign” – probably more harmful than helpful [Gussow]
- In fact, in 2009, there were
Polypharmacy – Juurlink
- Trimethoprim/sulfamethoxazole and ace-inhibitors/angiotensin receptor blockers, used in combination can lead to hyperkalemia and, in some cases, death [Juurlink et al]
- Acetaminophen, at just 2 grams/day, can elevate the INR in patients on warfarin [Pinson]. Acetaminophen is still probably the analgesic of choice, but something to be aware of
Sepsis
- Lactate is not a measure of tissue hypoxia/anaerobic metabolism [Marik et al]
- Too much fluid is not a good thing = iatrogenic salt water drowning [Marik et al]
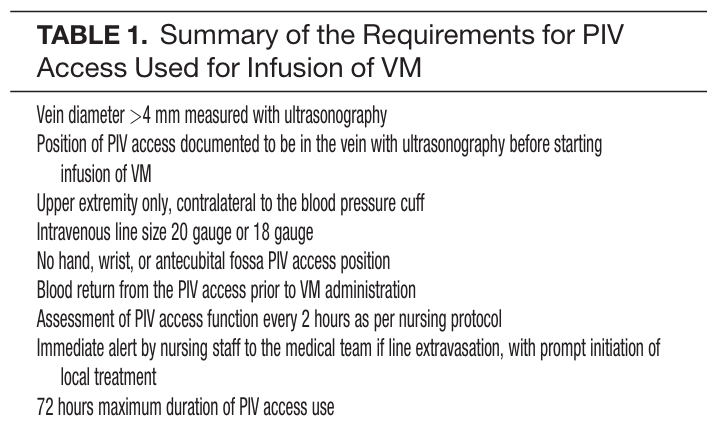
- Patients may need vasopressors. If they do, don’t delay based on central access. Vasopressors are ok through good peripheral lines for a day or so. [Loubani et al, Mayo et al] However, we should probably place the lines when we’re safely able.
- Of note, this does require strict protocols. Ex: Mayo study had stringent inclusion criteria