(ITUNES OR LISTEN HERE)
The Free Open Access Medical Education (FOAM)
We review the American Academy of Pediatrics guideline on Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk Infants.
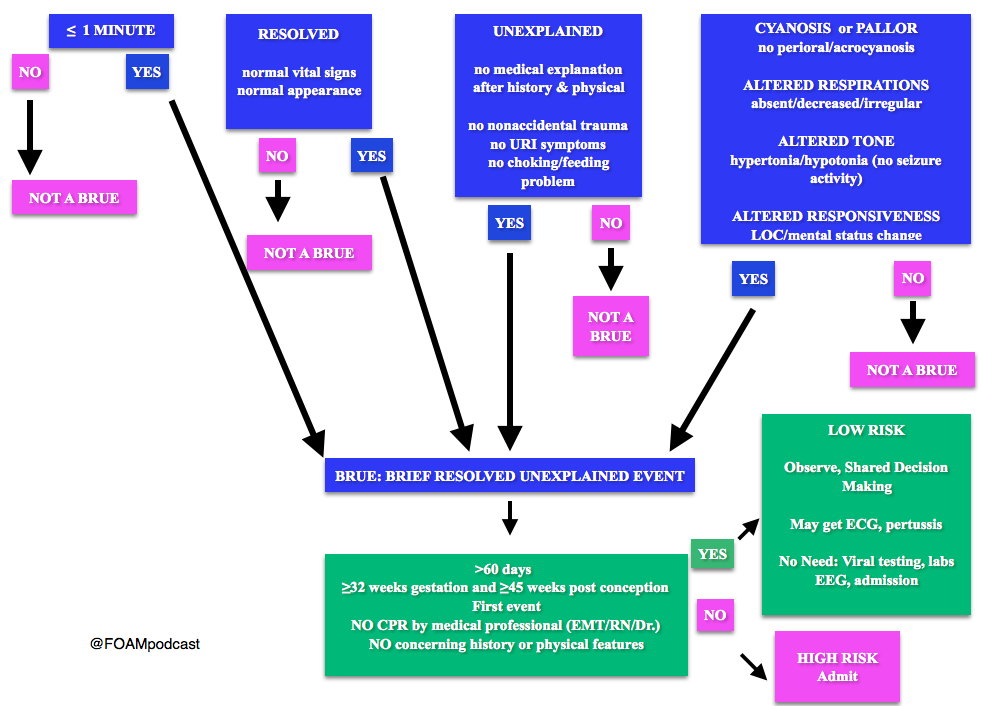
Note: Some have voiced concerns that these guidelines potentially downplay the event. The concern is that the yield of these workups and admissions may be low, but possibly worthwhile. At FOAMcast, we are not qualified to critique these guidelines but there are helpful tables and charts in them to realize that these recommendations really are only for specific events and children AFTER thorough history and physical.
Generously Donated Rosh Review Question
A 6-week-old boy is brought to the emergency room because of cyanosis. He was sleeping comfortably in a supine position right after a feeding when he suddenly choked, became limp and lips turned blue. The mother witnessed the event and blew to the face of the boy. The whole episode lasted for about two minutes. EMS was called and upon arrival at the house, the boy was back to his usual self. At the ER, he boy has normal vital signs with normal physical examination findings.
A. Admit for cardiorespiratory monitoring
B. Discharge after reassuring the parents
C. Observe for four hours in the ER
D. Request for complete blood count
[accordion]
[toggle title=”Answer” state=”closed”]
A. Admit for cardiorespiratory monitoring. The boy in the vignette had an apparent life-threatening event (ALTE) which is not a specific diagnosis but a description of an acute, unexpected episode that is frightening to the caretaker. ALTE includes one or more of the following features: apnea, color change (may be cyanotic, pallid, erythematous or plethoric), marked change in muscle tone (limpness or rigidity) and choking or gagging. A specific cause for ALTE can be identified in over one-half of patients after a careful history, physical examination, and appropriate laboratory evaluation. The remaining cases are considered idiopathic if no cause can be identified after a thorough assessment. Common etiologies for ALTE include gastroesophageal reflux, neurologic problems (such as seizures), and respiratory infection. The history of an ALTE must be taken seriously, even if the infant appears entirely well by the time he or she is evaluated. In-hospital observation with cardiorespiratory monitoring is indicated for infants whose initial evaluation suggests physiologic compromise. Hospital admission may provide important clinical information where additional episodes may be witnessed by medical personnel during the observation period. In addition, serious underlying medical conditions may become apparent. Discharging the patient after reassuring the parents (B) and observing the patient for four hours in the ER (C) are not appropriate management strategies for the infant in the vignette who needs admission for cardiorespiratory monitoring. Requesting for complete blood count (D) is not routinely done in the evaluation of an ALTE and would not aid in the management for the infant in the vignette.
[/toggle]
[/accordion]
References:
Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk Infants: Executive Summary. Pediatrics. In Press
A very timely podcast. We’ve just done a blog post on the same set of guidelines (http://dontforgetthebubbles.com/brue-is-the-new-black/) but it will be interesting to see if they translate over to us in Australia.
I think you highlighted one really important piece of information and that was about treating the parental anxiety. Recommending CPR training may not help in the acute setting and often the child may need admission just to reassure the parents (though they do not necessarily need a huge work-up). I think CPR training should be mandatory for all who by a home apnoea monitor, otherwise what is the point?
The team at the Children’s Hospital at Westmead in Sydney, Australia have come up with an excellent on-line learning package for parents (http://dontforgetthebubbles.com/cpr-training-for-parents/) that may help.
Keep up the good work as always. FOAMcast helped me pass my final Fellowship exam so will always have a special place in my heart.