FOAMcast brings you pearls from conferences we attend and presently it’s the American College of Emergency Physicians annual meeting, ACEP15 in Boston.
Jeremy Hoffman and Rick Bukata summarize recent, relevant literature each year (recently known as #hofkata). This year, our top three favorite
Dr. Jeff Kline (@klinelab) spoke on pulmonary embolism.
High Risk PE? Consider lysis (this is controversial, we are simply reporting Dr. Kline’s talk)
Size and location. Massive and proximal= bad
SBP <90 for more than 15 min OR 40mmHg drop from baseline
Signs of RV strain – echocardiography showing RV dilation OR hypokinesis?
Elevated troponin or BNP
ECG findings suggestive of cardiac strain: sinus tachycardia, incomplete right bundle branch block, complete right bundle branch block, T-wave inversion in leads V1 – V4.
Kline also participated in a knowledge translation workshop where he argued that sub-segmental PEs, without DVT on ultrasound, are NOT a real thing. This is controversial but he also argued that treating these is associated with harm [Carrier et al]
Jane Brody wrote an article, “What Comes After the Heimlich Maneuver” that ran in the NY Times and stirred up a ruckus on Twitter. This is a reasonable article on choking and details the limitations of the Heimlich maneuver. Unfortunately, the article ends instructing the layperson do to a cricothyrotomy (cric) with a sharp knife and “something like a straw or casing of a ballpoint pen (first remove the ink cartridge). “
Dr. Seth Trueger (@MDaware) wrote a post, Bad Idea Jeans, discouraging this practice saying that deciding which patient needs a cric is one of the more difficult but more important parts of this procedure.
On another note, our friend Dr. Andy Neill has found that medical students are able to perform crics with Papermate pens on cadavers [1]. However, it appears that most pens may not be suitable [2]. Further, while medical students are nearly lay people, we do not think this the cric should be within the domain of lay people (especially without patients already declared dead and preserved).
Cricothyrotomies – In reality, this is a bloody procedures that should only be done by those with proper training when the airway cannot be otherwise secured. The actual procedure has been detailed by those far smarter and with more experience than the FOAMcast crew. We recommend checking out Dr. Scott Weingart’s compilation of resources here.
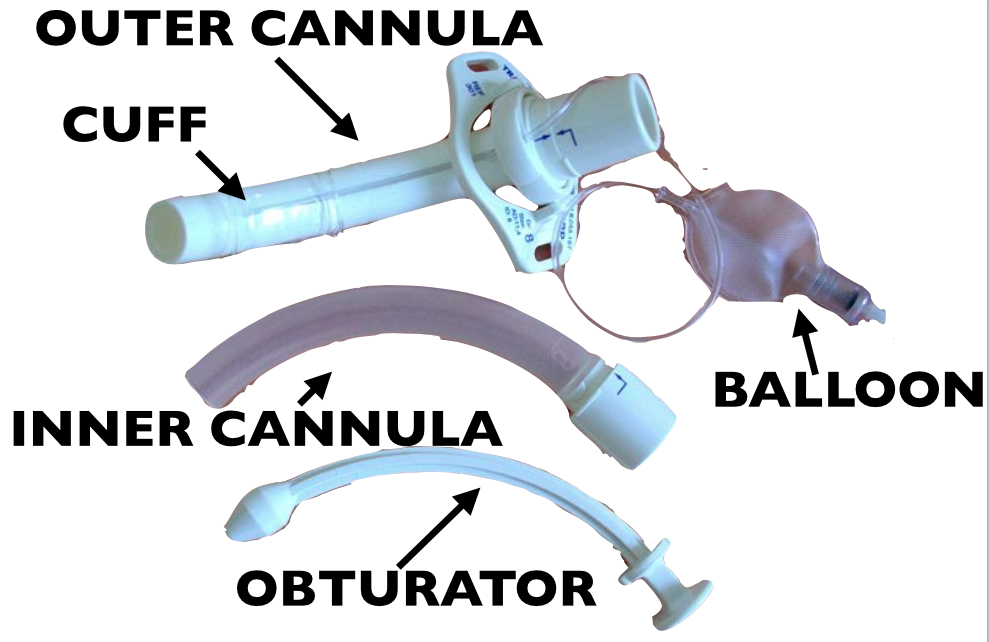
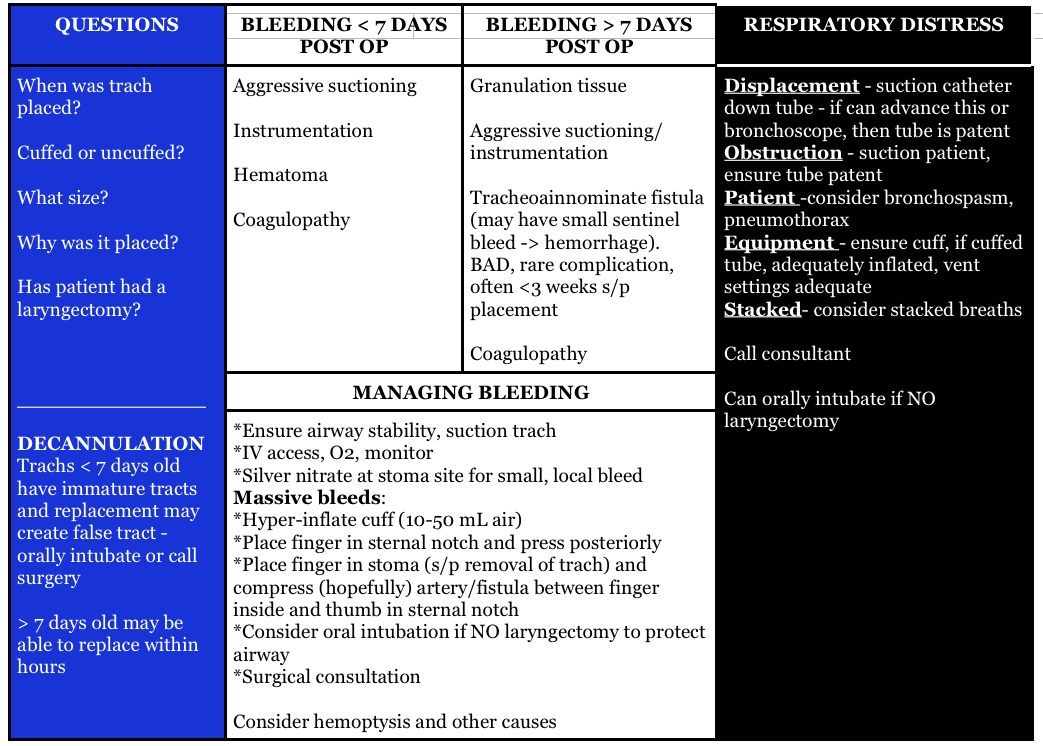
Question 1. A 72-year-old man who is 1 week out from an ischemic stroke presents with respiratory distress. He had a tracheostomy placed 6 days ago for sudden respiratory failure. The patient is hypoxic and tachypneic on presentation with minimal breath sounds bilaterally. There is no subcutaneous air around the stoma.[polldaddy poll=9110296]
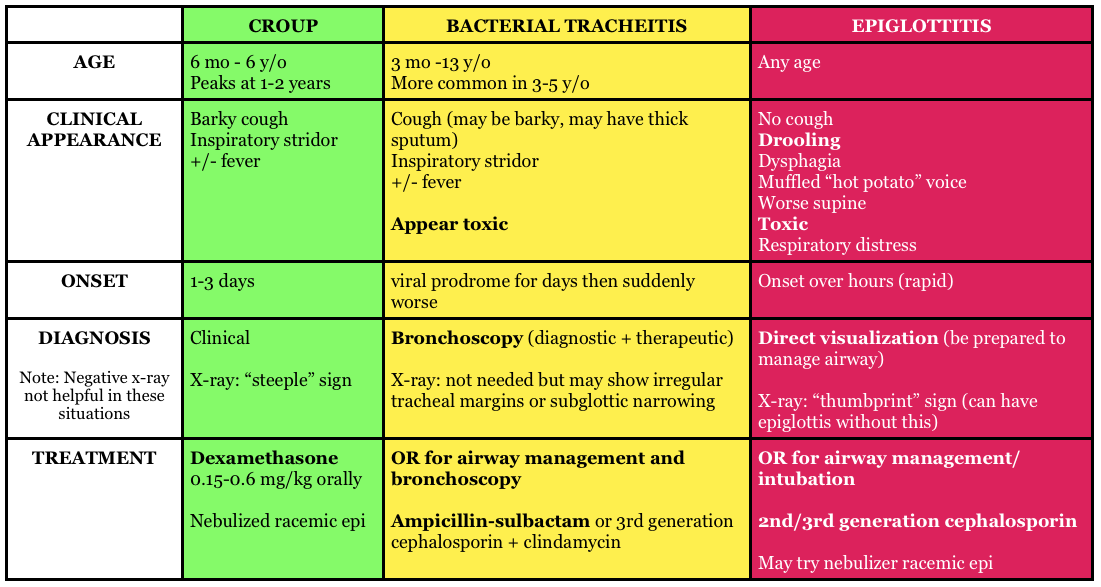
Question 2. A 3-year-old boy presents in severe respiratory distress. His mother informs you that he has been ill for the last 5 days, initially with a low-grade fever and “barky cough.” He was seen at an urgent care facility 4 days ago and given a “breathing treatment” and discharged on steroids. He has become progressively worse despite compliance with the steroid regimen, which prompted his mother to call an ambulance this morning. He is otherwise healthy and up-to-date on his immunizations. On examination, the child is toxic in appearance and febrile. His oropharynx is clear. You hear both inspiratory and expiratory stridor. [polldaddy poll=9110301]
Answers
1.The patient’s presentation is concerning for airway obstruction and the first step in management is suctioning of the tracheostomy tube. Tracheostomy tubes are placed for long-term mechanical ventilation in patients with anticipated prolonged or permanent respiratory failure. The two most common complications are obstruction and dislodgement. Sudden onset of respiratory failure often indicates mucous plugging or equipment failure. Suctioning of the tracheostomy is a simple procedure that may quickly relieve the patient’s symptoms. 2 to 3 ml of normal saline should be instilled into the tube followed by suctioning. Patients with slower decline in respiratory status may have a worsening of their underlying pulmonary pathology or may have developed a pulmonary infection. A cricothyrotomy (A) will not lead to effective oxygenation or ventilation as the cricothyroid membrane is above the tracheostomy site. The tracheostomy tube should not be removed and replaced with either an endotracheal tube (C) or a new tracheostomy tube (B) at this time because the tracheostomy tract has not matured at 6 days (this usually occurs at 15-30 days). If equipment failure in the form of a tracheostomy tube malfunction is suspected, the tube should be replaced with fiberoptic visualization to ensure that a false lumen isn’t created.
2.The patient is suffering from acute bacterial tracheitis. Bacterial tracheitis is the result of severe inflammation of the epithelial lining of the trachea leading to thick mucopurulent secretion production. This clinically manifests as viral prodrome with fever, URI symptoms, barky cough and stridor that intensifies and progresses to include a toxic appearing child with signs of airway obstruction, inspiratory and expiratory stridor, cyanosis, and severe respiratory distress. Another clue is that the child has been treated with medications (aerosolized epinephrine and steroids) for croup and has not improved clinically. Bacterial tracheitis is most common in children between the ages of 3 to 5 years. Most patients require orotracheal intubation for respiratory distress and ICU admission. The patient should be started on broad-spectrum intravenous antibiotics. Croup (B) is the most common cause of upper airway distress and obstruction in children between 6 months to 6 years of age with peak incidence at 2 years of age. Croup begins as a prodrome of low-grade fever and URI symptoms and is characterized by a barky cough, inspiratory stridor, and hoarse voice. Children are less toxic in appearance and rarely develop respiratory failure. The mainstays of treatment are steroids and aerosolized epinephrine. Epiglottitis (C) is characterized by abrupt onset of fever and sore throat and children classically present with difficulty in breathing, anxiety, stridor and drooling. This is less common in vaccinated children, such as the patient above and typically occurs in slightly older children. There is generally not a prodrome associated with epiglottitis. Peritonsillar abscess (D) occurs more commonly during adolescence and presents with trismus, unilateral sore throat, fever, tonsillar asymmetry, and uvula deviation away from the affected tonsil. The age of this patient and normal oropharynx examination make this diagnosis very unlikely.
References:
Neill A, Anderson P. Observational cadaveric study of emergency bystander cricothyroidotomy with a ballpoint pen by untrained junior doctors and medical students. Emergency medicine journal : EMJ. 30(4):308-11. 2013. [pubmed]
Owens D, Greenwood B, Galley A, Tomkinson A, Woolley S. Airflow efficacy of ballpoint pen tubes: a consideration for use in bystander cricothyrotomy. Emergency medicine journal : EMJ. 27(4):317-20. 2010. [pubmed]
The St. Emlyn’s team ran a post on the REVERT trial, which added a new spin to the traditional (and traditionally ineffective) Valsalva maneuver for stable supraventricular tachycardia (SVT). In this post, Dr. Rick Body goes through the trial covering not only the results but also drops pearls on methodology.
Randomized 433 patients with SVT to one of the following:
“Modified” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec and then placed supine with passive leg raise immediately after procedure (see video)
“Standard” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec while maintaining upright position
43% of the patients in modified Valsalva group versus 17% in the standard technique achieved sinus rhythm at one minute yielding an absolute risk reduction of 26.2% (p<0.001) with a number needed to treat of about 4 (3.8).
Core Content – Supraventricular Tachycardia (SVT) and Ventricular Tachycardia (VT)
Tintinalli (7e) Chapter 22; Rosen’s Emergency Medicine (8e) Chapter 79
SVT
Broad term referring to tachycardias originating above the ventricles, including the regular rhythms of sinus tachycardia, AV nodal reentrant tachycardia, AV reentrant tachycardia, and the irregular rhythms of multifocal atrial tachycardia, atrial fibrillation, and some forms of atrial flutter.
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients-
Valsalva maneuver – we like this method of having a patient blow on a syringe. Unfortunately, prior to the REVERT trial, the valsalva maneuver success rate has been documented ~19% [3].
Adenosine (0.1mg/kg or 6 mg in adult; 2nd dose 0.2 mg/kg or 12 mg in adult, with occasional dose adjustments) – administration can be tricky because of the drug’s short half life, necessitating proximal administration, elevation of the arm, and a quick saline flush afterwards. You can combine the adenosine IN the flush as detailed in this post, meaning no stopcock.
Calcium channel blockers or beta-blockers (verapamil, diltiazem or even metoprolol, esmolol) – Recently the calcium channel blockers have increased in popularity in the FOAM world and these are Rosenalli approved [4,5].
Diagnosis: Typically wide QRS complex (95% with QRS >120 ms) and fast (150-200 beats per minute).
SVT with abberency can have a wide complex but this should be treated as VT [4,5] (see this video)
Monomorphic – complexes have same morphology
Polymorphic – complexes of various morphologies, associated with poor prognosis [4,5]
Treatment:
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients with monomorphic VT–
Electrical cardioversion
Procainamide – Level B recommendation for first line treatment of monomorphic VT[6].
Amiodarone – common in the US but per the AHA guidelines “reasonable in patients with sustained monomorphic VT that is hemodynamically unstable, refractory to conversion with countershock, or recurrent despite procainamide or other agents. (Level of Evidence: C)” [6].
Note: Dangerous if prolonged QT [6]
Lidocaine – “may be reasonable” [6]
Stable patients with polymorphic VT –
Electrical cardioversion
Beta-blockers (particularly if ischemic)
Amiodarone
Cardiac catheterization if potentially ischemic cause [6]
Torsades de Pointes – withdraw offending agent, magnesium sulfate IV if “a few episodes” per the AHA
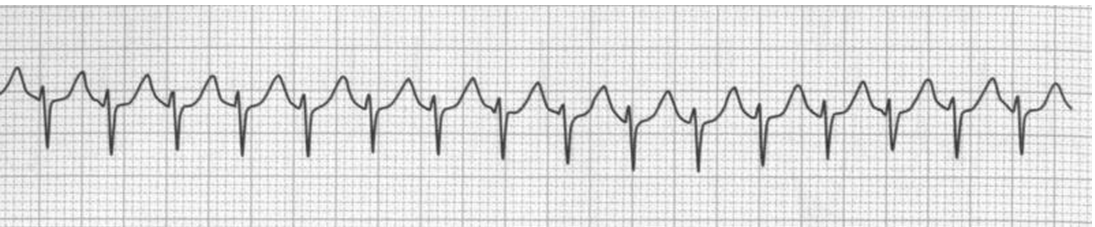
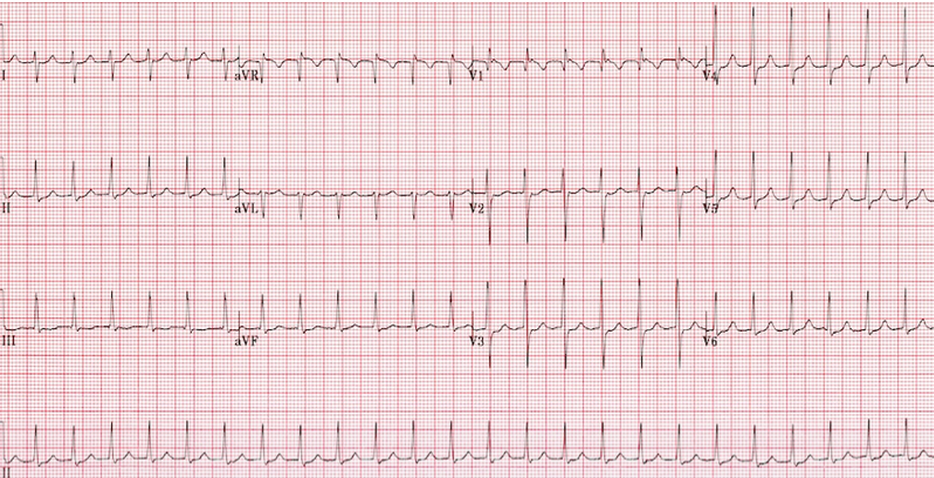
Question 1.A 26-year-old woman presents with dizziness and palpitations. She reports episodes of these symptoms beginning about 1 week ago, which initially only lasted a few minutes. However, for the past two days, she has had about 4 episodes a day which last about 20 minutes each. Her social history is significant for heavy caffeine intake. Her pulse is 166 bpm and her blood pressure is 140/70. Her rhythm strip is seen below. [polldaddy poll=9061960]
Question 2. A 33-year-old woman with chronic persistent asthma presents with palpitations. Her vital signs are HR 210, BP 118/73, and pulse oxygenation of 97% on room air. An ECG is shown below. [polldaddy poll=9061966]
Smith et al. Effectiveness of the Valsalva Manoeuvre for reversion of supraventricular tachycardia. Cochrane Database Syst Rev. 2013 Mar 28;3:CD009502. doi: 10.1002/14651858.CD009502.pub2
”Cardiac Rhythm Disturbances.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. pp 136-146.
This week we cover a post from Dr. Rory Spiegel, author of EMnerd, on initial nonoperative management of acute appendicitis based on an article by Salminen et al in JAMA 2015.
530 patients with CT confirmed acute, uncomplicated appendicitis were randomized to operative intervention (n=273 receiving open laparotomies) or non-operative intervention (n=257 receiving antibiotics).
27.3% (n=70, CI 22-33.2%) of patients who received medical management (ertapenem x 3 days then 5 days of levofloxacin) had an appendectomy by the 1 year mark
7 patients (2.7%) in medical management group had complicated appendicitis at one year, 0 had abscesses
45 patients (20.5%) in the operative group had surgical complications
This is a non-inferiority study where the intent is to demonstrate that an experimental treatment (antibiotics alone) is not substantially worse than a control treatment (immediate surgery). The authors set the non-inferiority margin at 24%, which means that a failure rate (appendectomy by 1 year) >24% would render medical management inferior.
Authors Conclusion: “Among patients with CT-proven, uncomplicated appendicitis, antibiotic treatment did not meet the prespecified criterion for noninferiority compared with appendectomy.”
Spiegel’s Conclusion: “there is a great deal to be determined before this non-invasive strategy can be considered mainstream practice…in what was once considered an exclusively surgical disease, the majority of patients can effectively be managed conservatively. Despite not meeting their own high standards for non-inferiority, the authors demonstrated that for most patients with acute appendicitis, when treated conservatively with antibiotics we can avoid surgical intervention without complications of delays to definitive care.”
More FOAM on non-operative treatment of appendicitis: The SGEM
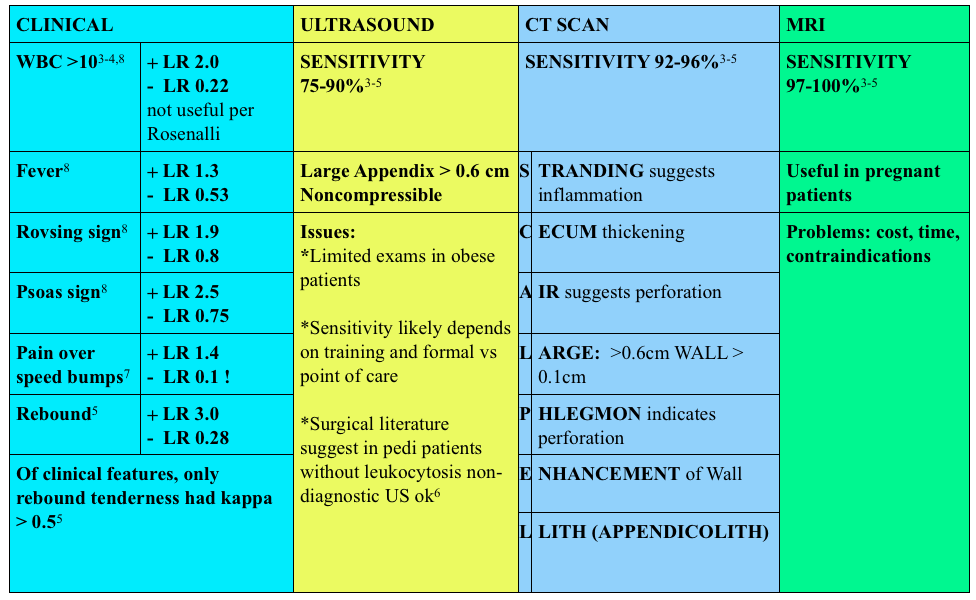
Use of contrast enhanced CT scans controversial. Rosenalli and the American College of radiology concur that oral contrast is probably not needed but does increase the emergency department length of stay [3-5].
Treatment:
Surgical consult
Antibiotics:
Broad spectrum beta-lactams: ampicillin-sulbactam 3g IV (75 mg/kg IV in peds) piperacillin-tazobactam 4.5g IV, cefoxitin 2g IV (40 mg/kg IV in peds) OR metronidazole 500 mg IV + ciprofloxacin 400 mg IV
Other things to consider in special populations in right lower quadrant:
1. A 22-year-old man presents with abdominal pain followed by vomiting for 1 day. His examination is significant for right lower quadrant tenderness to palpation. He has a negative Rovsing sign. [polldaddy poll=9026936]
2. A 22-year-old woman presents with lower abdominal pain and vaginal discharge. She is sexually active with men with inconsistent barrier protection. Her vitals are normal other than temperature of 101°F. On examination, there is yellow cervical discharge, no cervical motion tenderness, but uterine and left adnexal tenderness. An ultrasound does not show any evidence of tubo-ovarian abscess. [polldaddy poll=9026939]
Answers.
1. B. Sensitivity or the true positive rate measures the proportion of actual positives that are correctly identified as such. It is determined by dividing the number of true positives of the test by the number of true positives + false negatives. Tests with a high sensitivity are good for ruling out disease as the test has very few false negatives. A test with high sensitivity is advantageous as a screening tool as it misses very few people with the disease. The onset of pain before vomiting has been found to be as high as 100% sensitive in diagnosing acute appendicitis.Rovsing’s sign (D) (indirect tenderness) describes pain felt in the right lower quadrant upon palpation of the left lower quadrant. This sign signifies the presence of peritoneal irritation and has a sensitivity of 58%. Right lower quadrant pain (C) has a sensitivity of 81% and fever (A) has a sensitivity of 67%.
2.This patient presents with signs and symptoms consistent with pelvic inflammatory disease (PID) and should be treated with ceftriaxone 250 mg IM and 2 weeks of doxycycline. PID is an ascending infection beginning in the cervix and vagina and ascending to the upper genital tract. Neisseria gonorrhoeae and Chlamydia trachomatis are most commonly implicated. It can present with a myriad of symptoms although lower abdominal pain is the most common. Other symptoms include fever, cervical or vaginal discharge and dyspareunia. Pelvic examination reveals cervical motion tenderness (CMT), adnexal tenderness and vaginal or cervical discharge. Inadequately treated PID can lead to tubo-ovarian abscess, chronic dyspareunia and infertility. Due to the variable presentation and serious sequelae, the CDC recommends empiric treatment of all sexually active women who present with pelvic or abdominal pain and have any one of the following: 1) CMT, 2) adnexal tenderness or 3) uterine tenderness. Treatment should cover the most common organisms and typically consists of a third generation cephalosporin (ceftriaxone) and a prolonged course of doxycycline. Patients with systemic manifestations or difficulty tolerating PO should be admitted for management.Ceftriaxone and azithromycin (A) are used in the treatment of cervicitis or urethritis. Clindamycin (C) and metronidazole (D) are used in the treatment of bacterial vaginosis. References:
1.Salminen P, Paajanen H, Rautio T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015;313(23):2340
In a prior FOAMcastini, we covered the updated ACEP tPA clinical policy. As residents, we sought perspectives from experts, the FOAMcast brain trust (Drs. Anand Swaminathan, Ken Milne, Ryan Radecki, and David Newman). We (Jeremy) also interviewed Dr. Jerry Hoffman, faculty at UCLA.
In this interview, Dr. Jerry Hoffman, a public skeptic and author of peer reviewed critiques of tPA provides interesting perspective on more than thrombolysis but on the future of guidelines (referencing this paper) and science in Emergency Medicine.
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The plenary, facilitated by the brilliant Dr. Victoria Brazil, focused on the impaired provider. At SMACC we’ve heard time and time again – we are fallible, we make mistakes.
Dying – Dr. Ashley Shreves
What often presume what our patients want without asking them. When dying patients are asked what they want, it comes down to dignity. 1) Being clean 2) Naming a decision maker and then other top priorities essentially come down to healthcare providers listening [Steinhauser et al]
We don’t ask patients about their code statuses appropriately. First, we often spend almost no time doing this. One study of hospitalists found that code status discussions lasted, on average, one minute. Further, that one minute was spent mostly focused on procedures [Anderson et al]
Communicate!
Evidence Based Medicine – The consensus of these cage matches was that evidence isn’t all equal; the existence of data doesn’t necessarily mean it’s good data.
The Randomized Control Trial (RCT) has problems – Drs. Paul Young and Simon Finfer
Caution with Base Rate Neglect – we jump to inappropriate conclusions. For example, pretend you have tested positive for a typically fatal disease. The test is accurate 95% of the time. Most people would conclude that there was a 95% chance they have the disease – a death sentence. Yet, one would need to know the prevalence of the disease in the general population to determine the actual likelihood that the test was correct. If the prevalence of the disease is 1 in 1000, the likelihood that you actually have the disease based on this test is <2%.
We should read the primary literature, but we can’t read all of it. Use FOAM (judiciously) – Drs. Rory Spiegel and Ken Milne
Due to the volume of literature, we have to make some decisions on what to read (Systematic reviews? Meta-analyses? RCTs? Case Reports?)
Severe traumatic brain injury can cause apnea which leads to a spiral of hypoxia (and thus cell death) and hypercapnea (with cerebral vasodilation causing cerebral edema) which can result in poor neurologic outcome.
The key? Resuscitate these patients as a hypoxic arrest. These are patients that need an airway and need oxygen.
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The overarching theme to Day 1 at SMACC? Use your team- to keep you in check and for feedback. Our cases and errors are opportunities for reflection. Dr. Cliff Reid reminded us to follow up our patients and outcomes and learn from it all, without letting our egos get in the way. Dr. Simon Carley (St. Emlyn’s) gave a powerful talk on learning from mistakes later in the day; you will definitely want to listen to these when they come out.
The sub theme? Experts don’t need algorithms and tests. But the novices? That’s another story.
Trauma – Weingart. We won’t delve into his thoughts on ATLS here (hint: ATLS isn’t for experts).
Ignore the first automated blood pressure, it’s probably wrong. Get a manual blood pressure.
Giving 3 units of blood in one hour? Prepare for massive transfusion, that means FFP, platelets, everything
If you go down the massive transfusion pathways, give an ampule of calcium every 4-6 units of plasma to combat the transfusion induced hypocalcemia from citrate.
The Shock Index (HR/SBP), isn’t as exciting as we once thought. It may be a guide, but not reliably so.
Pain – Strayer
Analgesia doesn’t = opiates. Think about local analgesia.
Pain as the “5th vital sign” – probably more harmful than helpful [Gussow]
In fact, in 2009, there were
Polypharmacy – Juurlink
Trimethoprim/sulfamethoxazole and ace-inhibitors/angiotensin receptor blockers, used in combination can lead to hyperkalemia and, in some cases, death [Juurlink et al]
Acetaminophen, at just 2 grams/day, can elevate the INR in patients on warfarin [Pinson]. Acetaminophen is still probably the analgesic of choice, but something to be aware of
Sepsis
Lactate is not a measure of tissue hypoxia/anaerobic metabolism [Marik et al]
Too much fluid is not a good thing = iatrogenic salt water drowning [Marik et al]
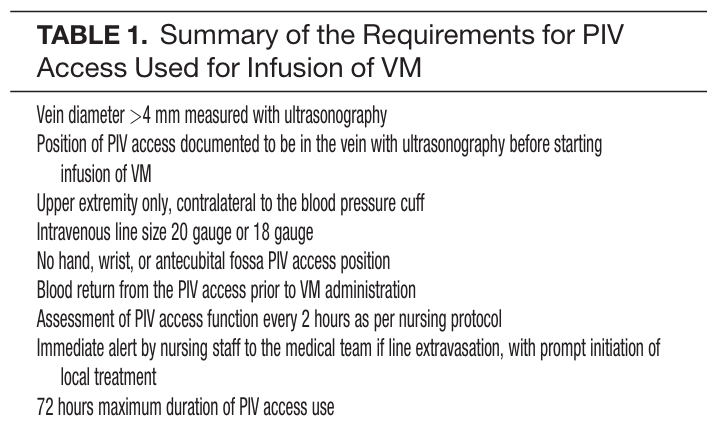
Patients may need vasopressors. If they do, don’t delay based on central access. Vasopressors are ok through good peripheral lines for a day or so. [Loubani et al, Mayo et al] However, we should probably place the lines when we’re safely able.
Of note, this does require strict protocols. Ex: Mayo study had stringent inclusion criteria
We enjoy contributing to the Free Open Access Medical education (FOAM) community. Creating FOAM is not free and requires significant costs in time and money. Yet, we find this investment invaluable and appreciate everyone who listens, as well as those who champion our endeavor (including the supportive people in our life that tolerate “FOAMcast dates” and tiptoe around whilst recording). We would also like to thank everyone who has contributed by means of post-publication peer review (Brett Schupack, Dr. Marc Probst, Dr. Gabriel Cade, Dr. Iain Beardsell, and countless others). Please continue to not only let us know when we get it right, but also when we get it wrong. We appreciate the suggestions, praise, feedback, and corrections.
Given our love of spaced repetition, we review our favorite pearls and mnemonics from the past year.
HANG IV: hernia, adhesions, neoplasm, gallstone (ileus), intussception,
Heart failure episode – treatment for right ventricular heart failure.
Optimize OHCRAP – Oxygenation, Hemodynamics, Contractility, Rate/rhythm, Afterload, and Preload
Headaches – Likelihood of migraine diagnosis (comes from the outpatient literature) = POUND. 4 criteria very indicative of migraine (+LR 24), 3 criteria also likely (+LR 3)
Pounding headache
hOurs: headache lasts 4-72 h without medication
Unilateral headaches
Nausea
Disabling: disrupts daily activities
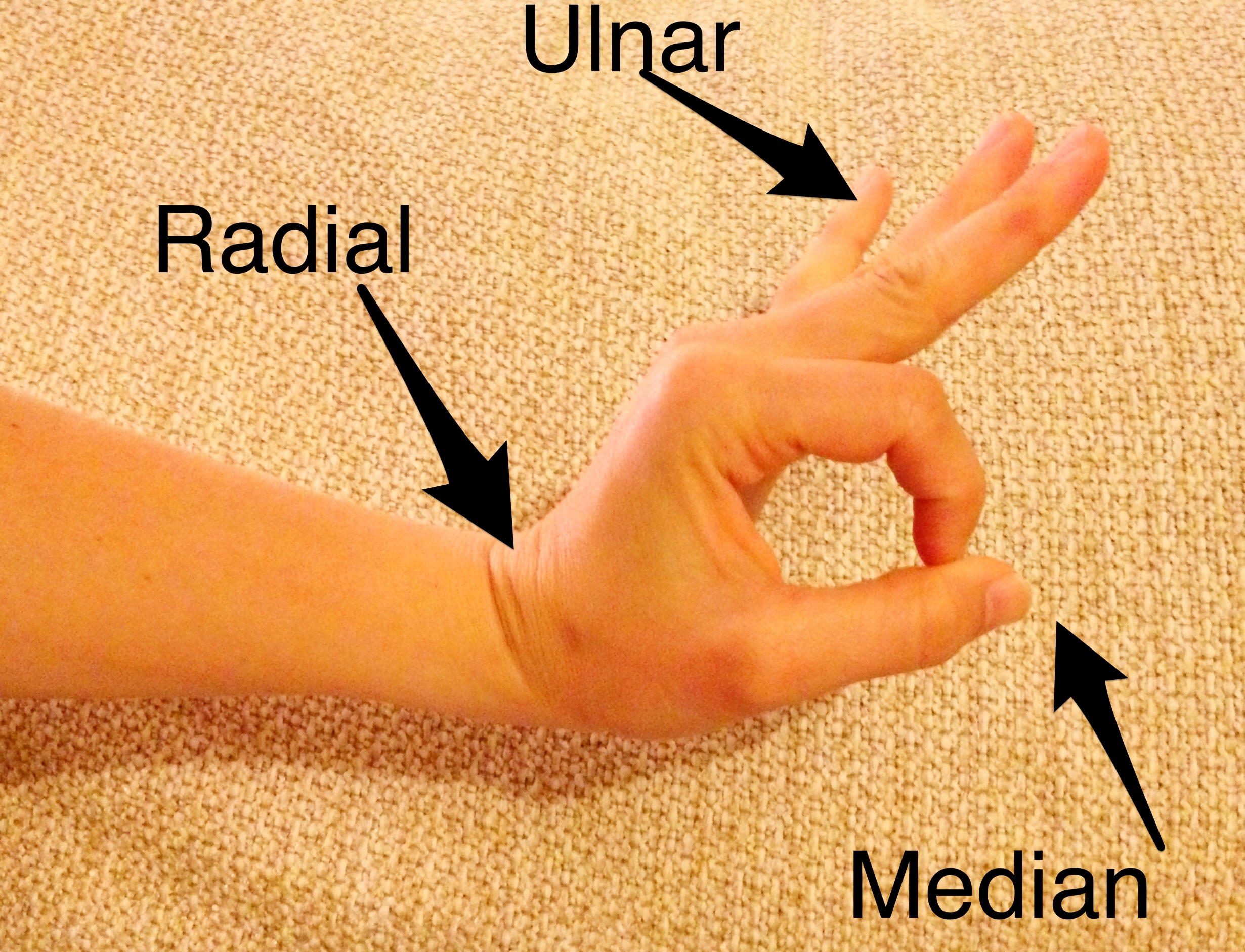
Our most frequently used clinical pearl:
The hand exam, in one movement:
Motor Exam of the Hand
Our favorite visual aid:
Burns – Grading the burn according to the Egyptian flag (because we all knew what that looked like).
Burn Degree
Worst visual aid: the Knee volcano (we won’t go there again)
Cord – complete cord syndrome that persists longer than 24 hours is highly unlikely to have any motor recovery. These patients need urgent intervention. This is we must differentiate between the complete and incomplete cord syndromes. Complete = “total loss of motor power and sensation distal to the site of the spinal injury.”
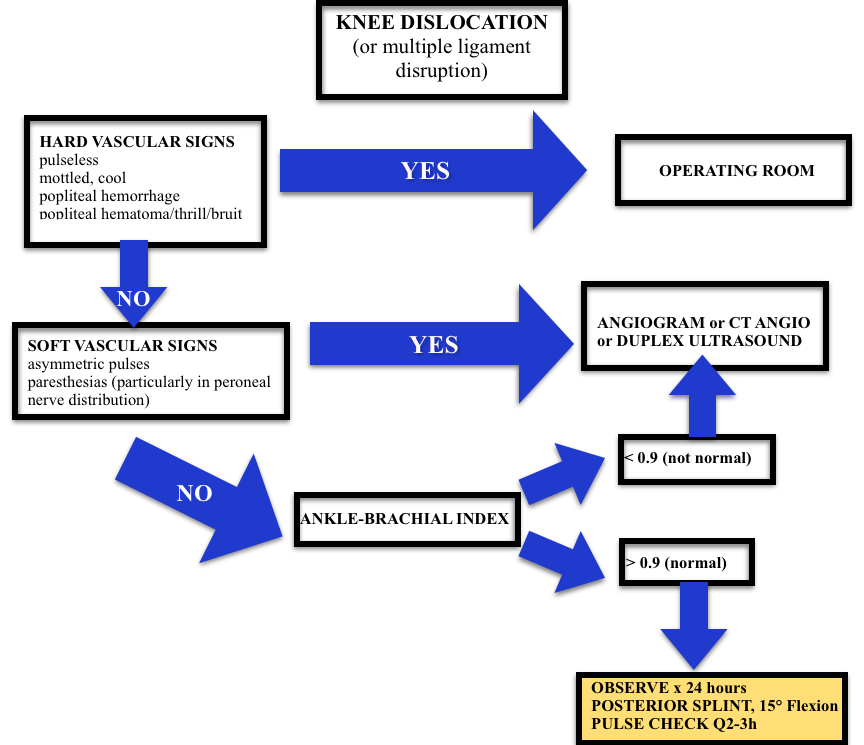
Knee/Leg– Beware knee dislocations. Of patients with popliteal disruption, the amputation rate rises to 90% 8 hours after the injury without surgical intervention.
Knee Dislocation Algorithm
Time is skin?
Hey Jeremy, re burns – surely needed a ‘Time is skin’?? @FOAMpodcast
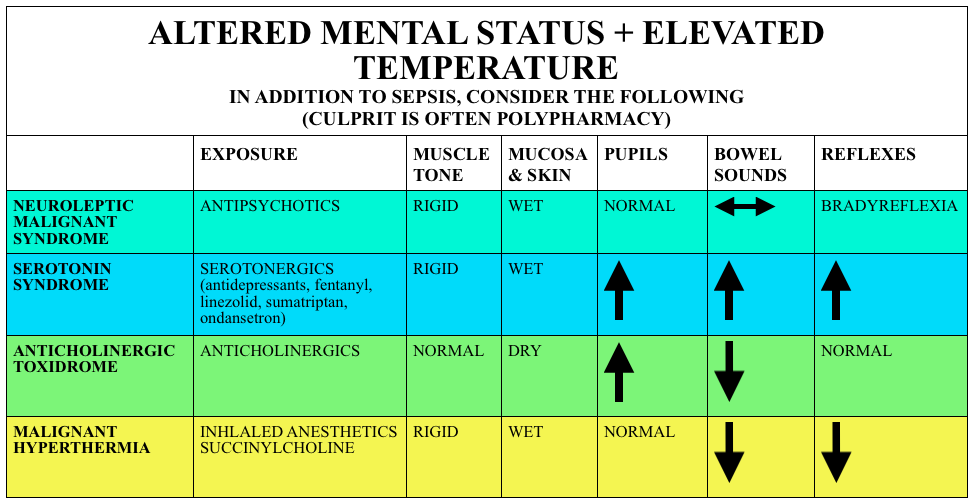
Malignant hyperthermia – a rare condition typically associated with volatile anesthetics, so more often an OR/inpatient issue; however, has been associated with succinylcholine use.
Cause: most often a mutation of the ryanodine receptor which, in the presence of certain anesthetics or succinylcholine causes too much intracellular calcium. This leads to increased ATP production.
Caution with calcium channel blockers – may lead to hyperkalemia or myocardial depression
Dantrolene has also been used in severe dinitrophenol (industrial chemical and weight loss supplement) toxicity – see this Poison Review post.
The Bread and Butter
We cover syndromes associated with psychiatric medications and polypharmacy including neuroleptic malignant syndrome (NMS), serotonin syndrome, and some extrapyramidal side effects. We do this based on Rosen’s Emergency and Tintinalli. But, don’t just take our word for it. Go enrich your fundamental understanding yourself.
Ref: Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352:(11)1112-20.
Neuroleptic Malignant Syndrome
Caused by atypical antipsychotics, rare, idiosyncratic and may persist for 2+ weeks after discontinuation of the offending medication
Symptoms – Varied diagnostic criteria but requires temp >100.4F + muscle rigidity + at least two of the following (in rough order of frequency):
Diaphoresis
Leukocytosis
AMS
Elevated creatine kinase
Labile blood pressure
Tachycardia
Tremor
Incontinence
Dysphagia
Mutism
Treatment – remove offending agents, supportive care (intravenous fluids, cooling), benzodiazepines. Dantrolene, amantadine, and bromocriptine are not recommended.
Serotonin Syndrome
(PV card from Academic Life in Emergency Medicine). Caution with the elderly as these symptoms may be attributed to infection or delirium (and vice versa).
Symptoms – Classical clinical triad of AMS + Autonomic instability (Hyperthermia, Tachycardia, diaphoresis) + Neuromuscular Abnormalities: Myoclonus, ocular clonus, rigidity, hyperreflexia, tremor. Yet like most clinical triads, this performs poorly. The Hunter Criteria are often used (Sensitivity ~84%):
Serotonergic agent plus 1 of the following:
Spontaneous clonus
Inducible clonus + agitation or diaphoresis
Ocular Clonus + agitation or diaphoresis
Tremor + hyperreflexia
Hypertonia + temp >38F AND ocular clonus or inducible clonus
Serotonin syndrome often begins with akathisia (restlessness) and body systems become increasingly “ramped up” with tremors, followed by altered mental status, and then incereasing amounts of rigidity (inducible clonus -> Sustained clonus (+/- ocular clonus) -> Muscular rigidity -> Hyperthermia -> Death)
Causes – While often associated with antidepressants, polypharmacy seems to be the culprit here. Serotonin syndrome is commonly associated with some of these medications
Question 1. A 35-year-old man presents with fever, hypertension and altered mental status. He was recently started on haloperidol for schizophrenia. Physical examination reveals a confused patient with muscle rigidity. [polldaddy poll=8842561]
Answers
1. C. FOAMcast editorial: This is an exercise in selecting the *best* answer, not the one that is most correct. You’ve probably noted that a benzodiazepine is not an option, the next best option is dantrolene.
This patient presents with signs and symptoms concerning for neuroleptic malignant syndrome (NMS) and should be treated with dantrolene. NMS is a life-threatening complication of neuroleptic drug treatment. It is rare and only effects 0.5 – 1% of patients receiving these drugs. Although it is more common with use of the typical neuroleptic medications, it can also be seen with the atypical agents. It usually occurs within the first few weeks of starting neuroleptic medications but can also be seen after an increase in dosage. NMS is characterized bymuscle rigidity, fever, altered mental status and autonomic instability. Muscle contraction leads to an elevated serum creatinine kinase. Due to similarities, the disease may be confused with serotonin syndrome. NMS can become complicated by respiratory, hepatic or renal failure, cardiovascular collapse, coagulopathy or gastrointestinal hemorrhage. Dantrolene is a direct acting muscle relaxant that can be beneficial in severe cases.
Temperature – often causing burns down to the level of the vocal cords, but not below.
Toxins – products of combustion such as cyanide, carbon monoxide, and hydrogen sulfide are asphyxiants and impair oxygen utilization
Irritants – inhaled particulates irritate airways
Airway edema peaks at 24-48 hours
Diagnosis made on bronchoscopy
Nebulized heparin, N-acetylcysteine, and albuterol protocol
May be beneficial, but protocols based on small studies. Rosen gives a head nod to this regimen, yet the evidence is questionable [1-3].
Nebulized heparin can be used at 10,000 international units every 4 hours, followed by nebulized NAC & albuterol 2 hours later for a total of 7 days.
Nebulized heparin may help prevent formation of airways casts.
NAC may have a mucolytic effect and help scavenge free radicals.
Albuterol added to prevent bronchospasm
Alternating nebulized heparin and NAC may:
Improve P/F ratio (not a patient centered outcome)
Decrease ventilator days
Reduce the development of acute lung injury
The Bread and Butter
We cover burns including nomenclature, fluid resuscitation, burn center referral criteria, and more. We do this based on Rosen’s and Tintinalli. But, don’t just take our word for it. Go enrich your fundamental understanding yourself.
Burn Depth
Classically, burns were described in degrees but are now described by the degree of thickness (except, apparently, fourth degree burns). At FOAMcast, we like to remember these distinctions by thinking about the Egyptian flag, with the flag pole representing fourth degree burn or burns essentially down to the bone.
Burn Degree
Fluid Resuscitation
The Parkland Formula is probably one of the most well known but both this formula and the modified Brooke formula have led to fluid “creep” or over-resuscitation, which may have lasting consequences. Major guidelines and Rosenalli approve another method, the “Rule of Tens.”
Question 2. A 52-year-old woman is brought to the emergency department with burns from a house fire. Physical exam reveals superficial burns over her entire left arm and partial-thickness and full-thickness burns covering her entire right arm, her anterior right leg and anterior trunk. [polldaddy poll=8824315]
Answers
1. C. Burn classification is based on burn depth. Second-degree burns are classified into superficial and deep partial-thickness burns. Deep partial-thickness burns extend into thereticular dermis. Skin color is usually a mixture of red and blanched white, and capillary refill is slow. Blisters are thick-walled and commonly ruptured and the skin may appear leathery white. Two-point discrimination may be diminished, but pressure and pinprick applied to the burned skin can be felt. Whereas superficial partial-thickness burns usually re-epithelialize 7-10 days after injury; so the risk of hypertrophic scarring is very small. For deep partial-thickness burns, tissue may undergo spontaneous epithelialization from the few viable epithelial appendages at this deepest layer of dermis and heal within 3-6 weeks. Because these burns have less capacity for re-epithelializing, a greater potential for hypertrophic scar formation exists. In deep partial-thickness burns, treatment with topical antimicrobial dressings is necessary to prevent infection as the burn wound heals. Contraction across joints, with resulting limitation in range of motion, is a common sequela. Splash scalds often cause second-degree burns.
2. B. The extent of burn size in this patient is 36% total body surface area. A thorough and accurate estimation of burn size is essential to guide therapy and to determine when to transfer a patient to a burn center. The extent of burns is expressed as the total percentage of body surface area. Superficial burns are not included in the burn assessment. For adult assessment, the most expeditious method to estimate total percentage of body surface area is the Rule of Nines. This method only takes into account partial-thickness and full-thickness burns. Each leg represents 18% total percentage of body surface area; each arm represents 9% total percentage of body surface area; the anterior and posterior trunk each represent 18% total percentage of body surface area; and the head represents 9% total percentage of body surface area. This patient has partial-thickness and full-thickness burns covering her entire right arm, her anterior right leg and anterior trunk, which calculates to 36%. The superficial burn on her left arm is not included in the calculation. According to the Rule of Nines, the percentage in this patient can be calculated as follows: entire right arm = 9%; anterior right leg = 9%; anterior trunk 18%. 9+9+18= 36%.
2. Kashefi NS, Nathan JI, Dissanaike S. Does a Nebulized Heparin/N-acetylcysteine Protocol Improve Outcomes in Adult Smoke Inhalation? Plast Reconstr Surg Glob Open. 2014;2:(6)e165. [pubmed]
3. Elsharnouby NM, Eid HE, Abou Elezz NF, Aboelatta YA. Heparin/N-acetylcysteine: an adjuvant in the management of burn inhalation injury: a study of different doses. J Crit Care. 2014;29:(1)182.e1-4. [pubmed]


{kind=link}