Episode 3 – Ear Emergencies (iTunes)
The Free Open Access Medical Education (FOAM) – SMART EM Pseudoaxioms 2 and Literature Update
The podcast reviews:
- Bullous Myringitis, a painful infection of the tympanic membrane, is typically caused by viruses, strep. pneumoniae and moraxella and, less commonly, mycoplasma. The boards have caught up with this. Check out this review by Mellick.
- PHANTOM-S trial: Use of the STEMO (Stroke Emergency Mobile – an ambulance with neurologist and a CT scanner for suspected strokes) reduced mean alarm-to-treatment time by 25 minutes (95% CI, 20-29; P < .001) without an appreciable neurologic benefit for this intensive intervention.
- An article by Gregg et al in the NEJM discussed incredible improvements in diabetes outcomes as a result of tight glycemic control. Dr. Newman asserts that much of this is secondary to dilution, as the definition of diabetes changed in 1997. This resulted in more people with less severe disease being diagnosed with diabetes.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapters 237; Rosen’s (8e) Chapter 92. A good read on common ear emergencies from EBMedicine…but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Bullous Myringitis
This is a painful infection characterized by bullae on the tympanic membrane (TM), which has a richly innervated outer epithelium (hence the severe otalgia). Patients may collect fluid behind their TM or have a concomitant otitis media.
Etiology: viruses, typical otitis media pathogens. Mycoplasma and chlamydia have been associated with bullous myringitis but the association is unclear and these are not the most common causes.
Treatment: pain control, pain control, pain control. Antibiotics are optional in most cases. But then again, antibiotics are not necessary in most cases of otitis media. Both Rosen and Tintinalli are on board with this.
Perforated Tympanic Membrane

Photo:Didier Descouens (Wikimedia Commons)
Etiology: infection, trauma (q-tips, instrumentation), changes in pressure (diving, flying)
Treatment: Keep the ear canal dry, follow up with ENT. Most of these patients can go home. If the injury is in the posteriorsuperior aspect of the TM or secondary to penetrating trauma, they should see ENT within 24 hours because they may have damage to the bones of the middle ear.
Auricular Hematoma
Etiology: Blunt trauma (often associated with boxing, fights, or termed “rugby ear“)
Treatment: Incision, drainage, and compression dressing/splint. Photo guide to repair.
Ototoxic Agents (great table in Tintialli 8 e, Ch 237, p1551)
Risk of hearing loss typically increases with exposure to medication (dose and length of use) and issues with clearance such as renal insufficiency may cause medications to hang around longer than anticipated or at higher levels.
Loop Diuretics: furosemide, bumetanide, ethacrynic acid
Salicylates (aspirin and quinine), NSAIDs
Antibiotics that end in -mycin or -micin: aminoglycosides (gentamicin), vancomycin, erythromycin
Chemotherapeutic agents: vincristine, vinblastine, cisplatin, carboplatin
Topical agents: ethanol, polymixin B, neomycin
Sudden Hearing Loss Differential Diagnosis
Occurs over the span of three days.
Differential Diagnosis categories for any ailment can be remembered by the mnemonic VINDICATE
- Vascular – sickle cell, polycythemia
- Infectious/Inflammatory – viruses (zoster oticus or herpes, EBV, CMV, mumps), syphilis, labyrinthitis, temporal arteritis
- Neoplasms – leukemia, masses, acoustic neuroma
- Drugs – loop diuretics, antibiotics that end in -mycin or -micin (aminoglycosides like gentamicin, vancomycin, erythromycin), salicylates and NSAIDs, chemotherapeutic agents (cisplatin, carboplatin, vinblastine, vincristine, and topical agents (ethanol, polymyxin B, neomycin)
- Iatrogenic/idiopathic – perforated TM, idiopathic endolymphatic hydrops (Meniere’s disease) – vertigo, hearing loss, tinnitus
- Autoimmune -granulomatosis with polyangitis (Wegener’s)
- Trauma – ruptured TM
- Endocrine – diabetes, high cholesterol
Necrotizing Otitis Externa (Malignant Otitis Externa) – an infection that can turn into osteomyelitis of the skull
Presentation: otalgia, headache, and swelling and tenderness around the ear particularly in the setting of a prolonged course of otitis externa. Diagnosis often requires CT scan to gauge involvement.
Epidemiology: Diabetics, immunocompromised
Etiology: Pseudomonas (90%)
Treatment: Pediatrics- imipenem or an aminoglycoside and an antispeudomonal penicillin. Adults – cephalosporin or quinolone
Dispo: Mild cases with good follow up can get oral quinolones as outpatients. More severe cases – admission, IV antibiotics, and perhaps surgical debridement.
Generously donated Rosh Review questions (scroll for answers)
Question 1.[polldaddy poll=8093105]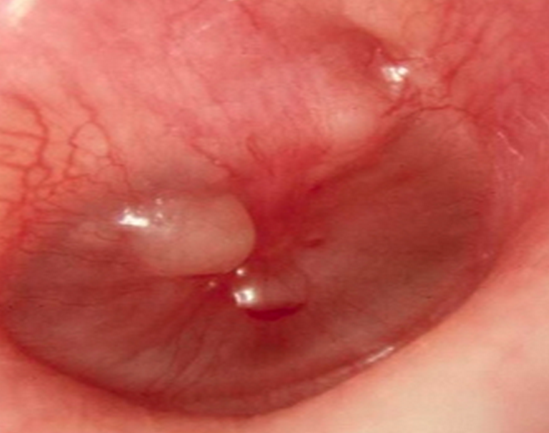
Question 2.
A 36-year-old woman presents to the ED complaining of decreased hearing and increased fullness to the right ear. Over the last week, she has used cotton-tipped applicators to attempt to remove cerumen from her right ear. On exam, you notice a cerumen-impacted external canal on the right. You irrigate the right ear with warm saline using an 18-gauge IV catheter and a plastic curette to remove the cerumen. During the procedure, the patient has sudden and complete hearing loss to the right ear. [polldaddy poll=8093098]
Question 3. A 16-year-old girl presents complaining of pain behind her left ear. She thought the pain was due to an ear infection and took three of her boyfriend’s leftover antibiotic tablets without seeing her primary care physician. Her ear pain improved for a couple of days, but now she is complaining of fever and discharge from the external auditory canal. Her vitals are T 38.4°C, BP 120/80, HR 108, and RR 18. On physical examination, she has postauricular tenderness, swelling, and erythema. You note purulent otorrhea through a perforated tympanic membrane. [polldaddy poll=8096505]
Answers:
1. D-Bullous myringitis was previously linked to Mycoplasma pneumoniae but it appears, based on middle ear aspirate culture results, that typical acute otitis media pathogens are the true cause. Among these, Streptococcus pneumoniae is most common.
2. C – The patient does not require admission (A) to the hospital. ENT care can be arranged for as an outpatient. Traumatic tympanic membrane perforations do not require otic antibiotics (B) unless the ear was contaminated such as from diving in seawater or the rupture is secondary to infection. The patient should receive more than ac otton ball (D) in her ear. Her management should include analgesia and ENT follow-up because complications of tympanic membrane rupture include facial nerve palsy, vertigo, and hearing loss.
3. C – This patient has necrotizing otitis externa.
References:
Silverberg M, Lucchesi M. Common Disorders of the External, Middle, and Inner Ear. Tintinalli’s Emergency Medicine, A Comprehensive Study Guide, ed 7. New York, McGraw-Hill, 2011, (Ch) 237:p 1556-1557.