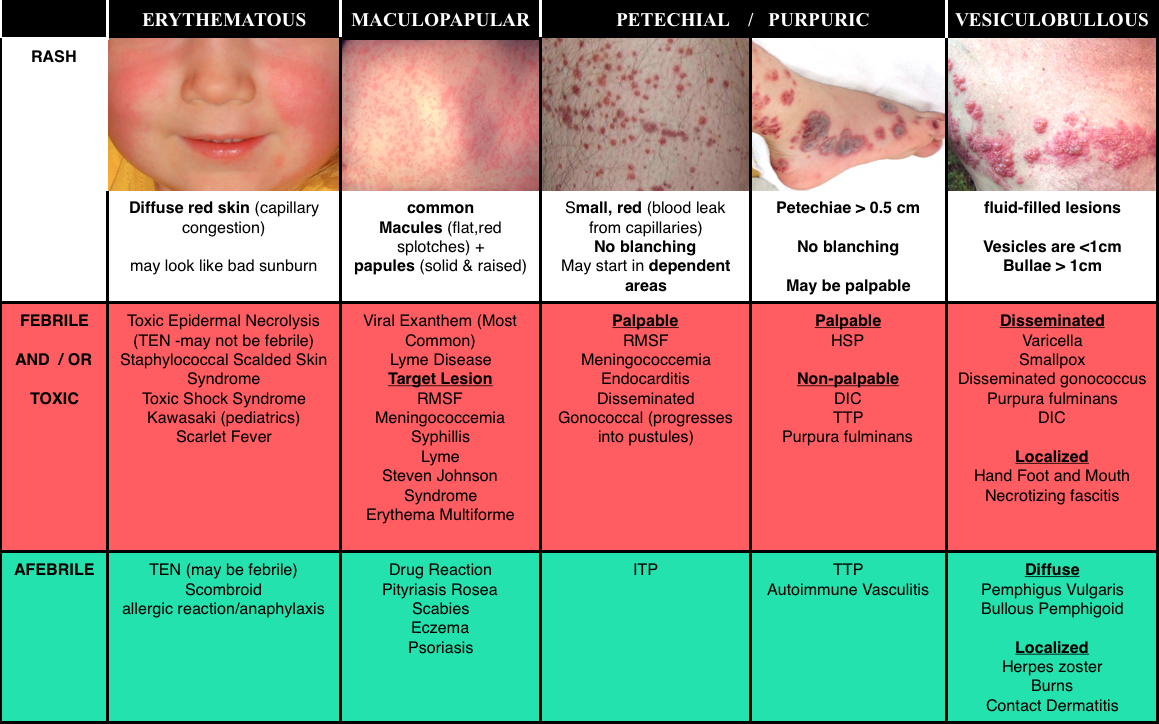
We cover several excellent post on rashes, including:
- Paucis Verbis Approach to Rashes – ALiEM
- Emergent Diagnosis of the Unknown Rash from EMJ
- What’s That Rash? – EMdocs
Core Content
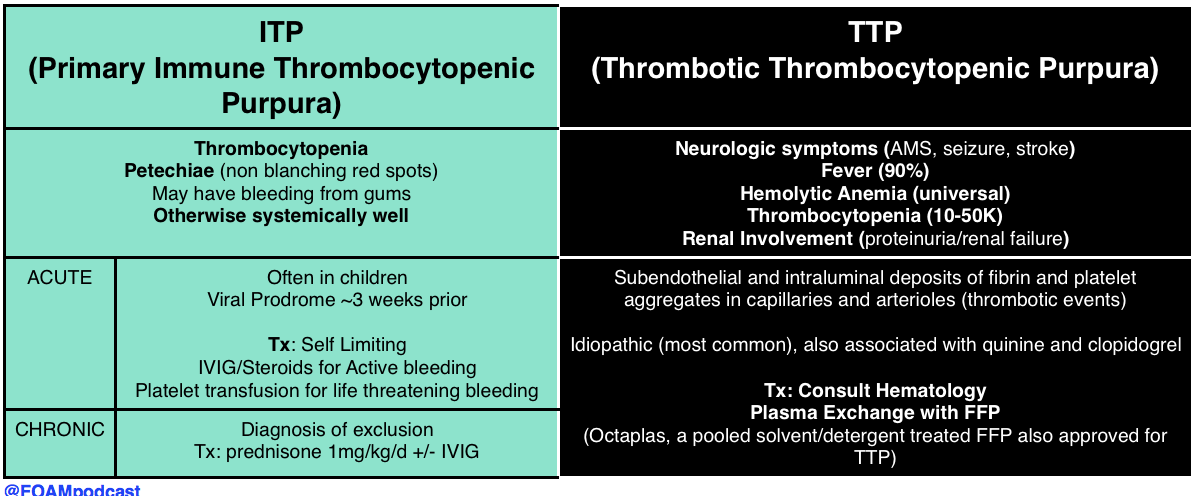
Next, we dive into core content on platelet problems including problems caused by drugs, immune thrombocytopenic purpura (ITP/idiopathic thrombocytopenic purpura) and thrombotic thrombocytopenic purpura (TTP) using Tintinalli Chapter 233 (8th ed) and Rosen’s Chapter 122 (7th ed) as a guide.
A previously healthy 3-year-old boy presents to the emergency room with bruising to his arms, legs, trunk, and face. The mother reports that the boy was well appearing yesterday and noted the bruising upon waking up this morning. She also noticed that his gums were bleeding while brushing his teeth before coming to the hospital. Mom denies any trauma but notes her son had a viral illness three weeks ago that kept him out of daycare. A complete blood count is notable for a white blood cell count of 7,000, hemoglobin of 12, and platelets of 10,000. Which of the following is the most likely diagnosis?
A. Idiopathic thrombocytopenia purpura
B. Leukemia
C. Thrombotic thrombocytopenic purpura
D. Wiskott-Aldrich syndrome
[accordion]
[toggle title=”Answer” state=”closed”]
A. Idiopathic thrombocytopenic purpura (ITP) is the most common cause of acute onset thrombocytopenia in an otherwise healthy child. It is most often seen in children aged 2-6 yearsand usually occurs 1 to 4 weeks after a viral illness. ITP is an autoimmune process where antibodies bind to the platelet surface. The platelet-antibody complex is then ingested by splenic macrophages and destroyed. The common physical exam findings are petechiae and purpura. If the child has hepatosplenomegaly, bone or joint pain, or lymphadenopathy, leukemia or other diagnoses should be suspected. In adolescents with new-onset ITP, systemic erythematous lupus should be suspected. Seventy to eighty percent of children will have spontaneous resolution of the symptoms. Treatment depends on the severity of the illness and includes such interventions as platelet transfusion for bleeding patients, steroids, and IVIG. Patients with ITP who have persistent or severe headache should undergo a head CT scan to rule out intracranial hemorrhage.

Leukemia (B) is rarely associated with thrombocytopenia alone and is typically seen with other cell lines being low with immature cells. In addition, physical examination may be remarkable for hepatosplenomegaly or lymphadenopathy. Children with leukemia often complain of bone pain. Leukemia is diagnosed by bone marrow biopsy and treated with chemotherapy. Thrombotic thrombocytopenic purpura (TTP) (C) is characterized by fever, micoangiopathic hemolytic anemia (MAHA), thrombocytopenia, abnormal renal function, and CNS changes. The microvascular thrombi are responsible for the clinical signs and symptoms. Lab findings associated with MAHA include anemia, schistocytes, spherocytes, and elevated reticulocytes. TTP is treated with plasmapheresis. Recurrent TTP is seen in patients with ADAMTS-13 deficiency. Wiskott-Aldrich syndrome (D) is an example of congenital thrombocytopenia. It is characterized by thrombocytopenia, small platelets, recurrent infections, and eczema. This disorder is X-linked.
[/toggle]
[/accordion]
A 9-year-old boy presents to the ED with bilateral knee pain, low-grade fever, nausea, vomiting, and diarrhea for the past 4 days. His vital signs are blood pressure of 116/80 mm Hg, heart rate of 98 beats per minute, respiratory rate of 14 breaths per minute, and a temperature of 38.1°C. On examination, you note the rash seen above. Urinalysis is positive for hematuria. Which of the following statements is the most accurate?
A. Despite plasma exchange, most patients progress to chronic renal impairment
B. Long-term prednisone therapy improves 5-year survival to greater than 50%
C. The disease is self-limited; most cases resolve within 6-8 weeks
D. Without treatment, the disease carries a mortality rate of 80% at one year
[accordion]
[toggle title=”Answer” state=”closed”]
C. The patient has Henoch-Schönlein purpura (HSP). This small-vessel vasculitis predominantly occurs in small children. Most cases follow an upper respiratory tract infection. HSP classically presents with fever, abdominal pain, arthritis, hematuria, and a pathognomonic round, palpable, symmetrical rash that appears on the dependent areas of the legs and buttocks. NSAIDs, dapsone, and prednisone have all been shown to relieve symptoms. The course of disease is typically self-limited. Most cases resolve within 6 to 8 weeks, with a recurrence rate of up to 33%.

Plasma exchange (A) has been found to be successful in the treatment of microscopic polyangiitis. In HSP, most patients do not progress to chronic renal impairment. Prednisone (B) therapy has increased the 5-year survival rate to greater than 50% in Churg-Strauss Syndrome, which is typically associated with fever, weight loss, malaise, and pulmonary symptoms, but it does not affect survival in HSP. Granulomatosis with polyangiitis (D), not HSP, once carried a 1-year mortality rate of 80%, however, the combination of cyclophosphamide and corticosteroids has been successful in inducing remission in more than 90% of patients.
[/toggle]
[/accordion]