We tackle some free open access medical education from the CDC on the flu vaccine, including:
- Recommendations that individuals with any severity of egg allergy (including anaphylaxis) receive the flu vaccine. The only modification that needs to occur is patients with a history of true anaphylaxis to eggs should be given the flu shot in a setting where they can be monitored by a healthcare professional if needed (i.e. a doctor’s office) [1]
- It is very unlikely that the flu vaccine causes Guillan-Barre Syndrome (GBS). If there is any increase as a result of the flu shot, it is 1-2 in 1,000,000 [1]
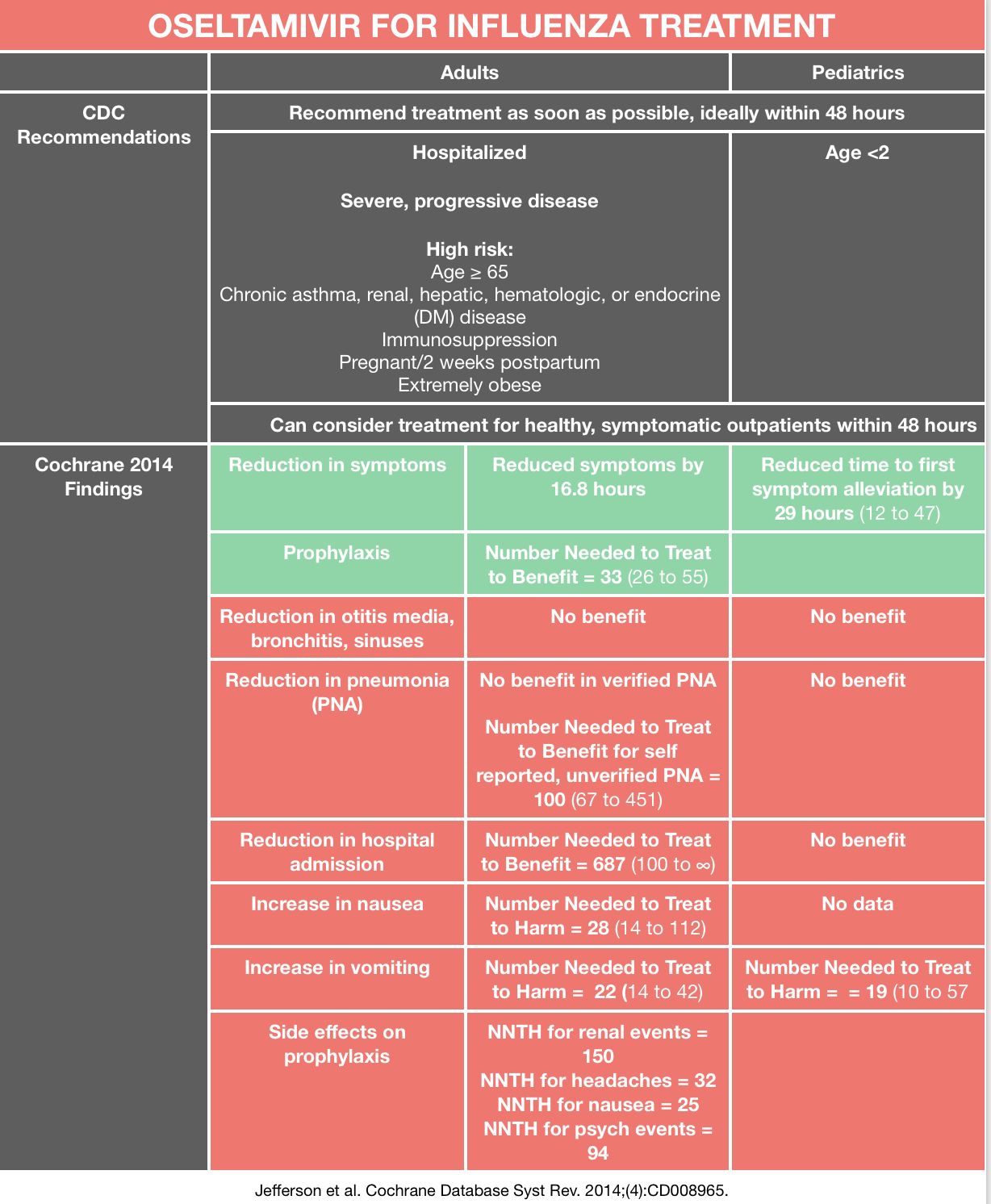
Oseltamivir for Influenza
We review the CDC recommendations as well as evidence from a 2014 Cochrane Review [1,3]. The data from the most recent Cochrane review includes studies from Roche Pharmaceuticals (makers of oseltamivir) that were initially unpublished and only released with international pressure, and seemingly do not support the CDC recommendations.
Rosh Review Emergency Board Review Questions
A 74-year-old woman presents with complaints of fever, productive cough with bloody sputum, shortness of breath, and headache. These symptoms developed and worsened drastically over the past 3 days. She recently recovered from an influenza infection 1 week ago. Her medical history otherwise includes only well-controlled hypertension. Vital signs on presentation are as follows: T 39°F, HR 106, BP 110/75, RR 30, oxygen sat 95% RA. A chest radiograph is obtained and a subsequent CT scan of the chest demonstrates multiple cavitary lung lesions. Which of the following organisms is most likely responsible for this patient’s presentation?
A. Clostridum perfringens
B. Escherichia coli
C. Mycobacterium tuberculosis
D. Staphylococcus aureus
[accordion]
[toggle title=”Answer” state=”closed”]
- This patient’s presentation of pneumonia with multiple cavitary lesions on imaging is consistent with a post-viral secondary necrotizing pneumonia. The most common organism in necrotizing pneumonia, particularly after a viral upper respiratory infection, is S. aureus. Necrotizing pneumonia is known to be caused by a specific S. aureus strain that produces Panton-Valentine Leukocidin (PVL). Often, this infection and the ensuing pneumonia that develops, is preceded by an influenza infection. Typically this S. aureus strain is also methicillin resistant. A CT of the chest with contrast is useful in diagnosis, and empiric therapy should be initiated promptly (vancomycin or linezolid, piperacillin/tazobactam). Surgical intervention may be necessary if complications develop – such as septic shock, gross hemoptysis and empyema. The following should be considered in the differential diagnosis of pulmonary cavitation: necrotizing pneumonia, lung abscess, septic pulmonary embolism, fungal/mycobacterial infection, vasculitis, primary/metastatic tumor, rheumatoid nodules, congenital cysts. Defining characteristics of necrotizing pneumonia include: preceding influenza infection, rapid onset and progressive symptom worsening, decreased WBC count, airway hemorrhages, respiratory failure, necrotic destruction of lung parenchyma, high mortality rate. A preceding viral infection brings a large number of immune cells to the lung tissue, such that when secondary bacterial infection strikes, there is a catastrophic activation and destruction of immune mediators that damage lung tissue and lead to necrotizing pneumonia.
Clostridial gas gangrene is a highly lethal necrotizing soft tissue infection of skeletal muscle caused by toxin- and gas-producing Clostridium species. Clostridium perfringens (A), previously known as Clostridium welchii, is the most common cause of clostridial gas gangrene (80-90% of cases). Escherichia coli (B) is one of the most frequent causes of many common bacterial infections, including cholecystitis, bacteremia, cholangitis, urinary tract infection (UTI), and traveler’s diarrhea, and other clinical infections such as neonatal meningitis and pneumonia. Mycobacterium tuberculosis (C) causes cavitary lung lesions in the upper lobes and clinically manifests as hemoptysis, weight loss and night sweats. It does not have any clinical correlation with influenza.
[/toggle]
[/accordion]
References
- “Misconceptions about Seasonal Flu and Flu Vaccines”. CDC. Available at: https://www.cdc.gov/flu/about/qa/misconceptions.htm
- “Influenza Antiviral Medications: Summary for Clinicians.” CDC. Available at https://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm
- Jefferson T, Jones MA, Doshi P, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev. 2014;(4):CD008965.
One thought on “Episode 78 – Influenza”
Comments are closed.