The US Food and Drug Administration (FDA) recently released another warning for fluoroquinolones, this time regarding aortic dissection and aneurysm.
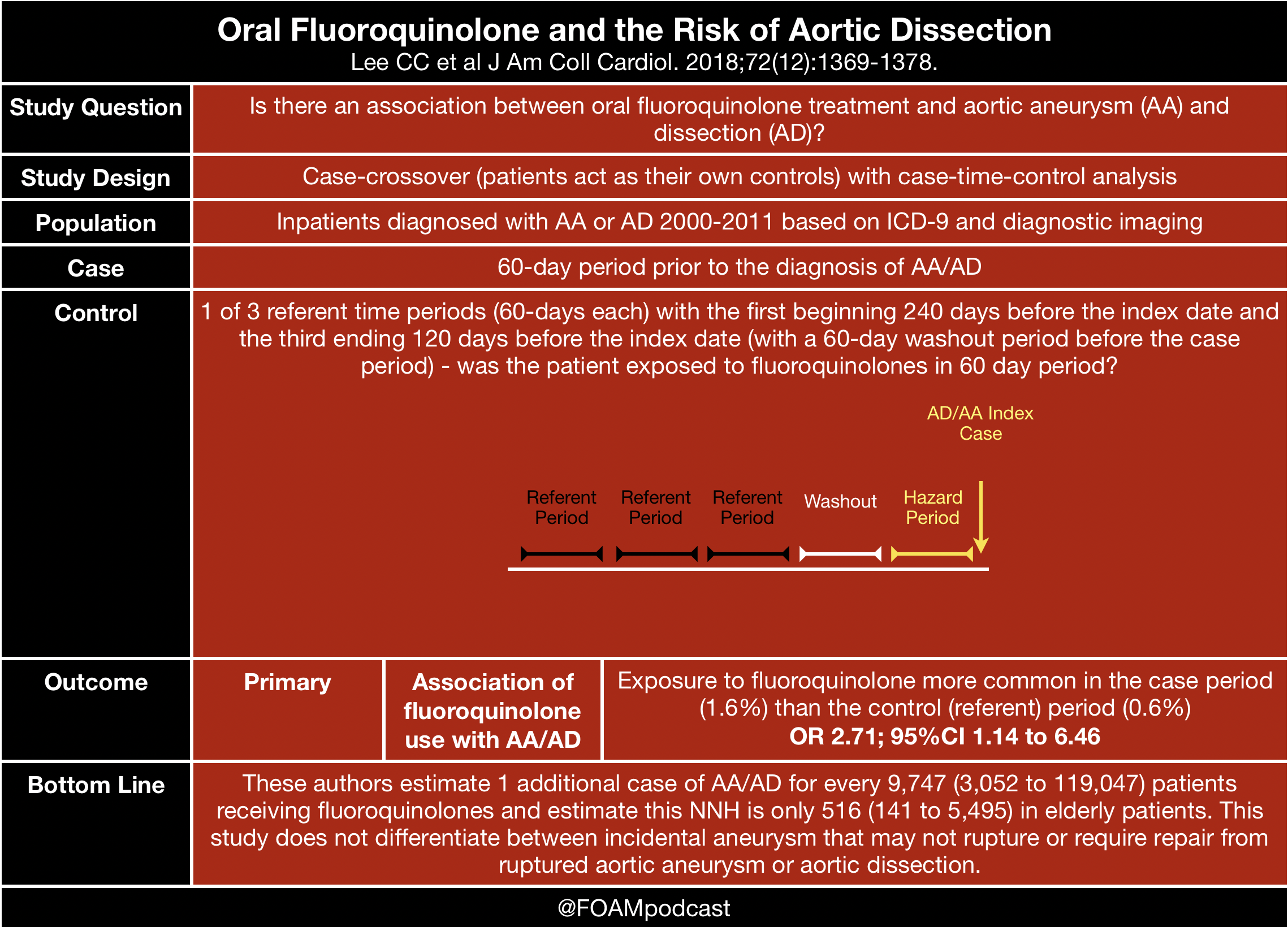
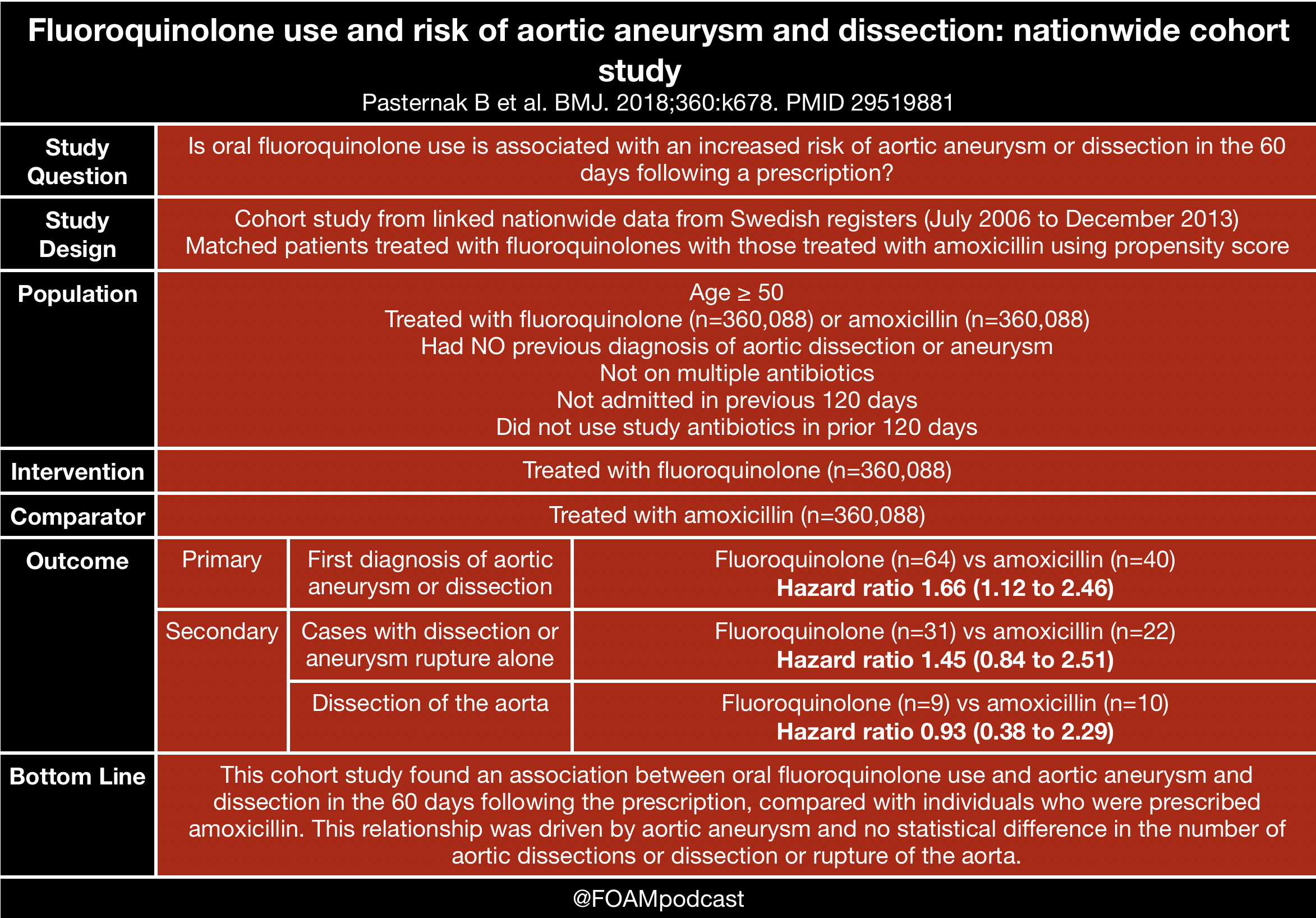
Much of the evidence behind this warning comes from these studies, released in 2015 and 2018 [1-3].
We also review the ACEP Clinical Policy on thoracic aortic dissections [4].

Check out Figure 1 cases on aortic dissection (free educational app for healthcare providers)

A 75-year-old man presents to the emergency department with acute onset of chest pain that radiates to his upper back. Which of the following features would help support a diagnosis of an aortic dissection?
A. A difference of 24 mm Hg in the systolic blood pressures between the upper extremities
B. An increase in heart rate of 120 beats per minute with standing
C. Auscultation of a carotid bruit
D. Chest pain that worsens with inspiration and improves with expiration
[accordion]
[toggle title=”Answer” state=”closed”]
A. An aortic dissection is relatively rare, but it can be life-threatening, so early diagnosis and intervention are critical. They occur more commonly in men aged 60 to 80 years old. Dissections occur secondary to tears in the aortic intima. They can develop due to trauma or degeneration of the aortic media. This deficit in the aorta causes blood to pass into the aortic media, which separates the intima from the surrounding media or adventia. A false lumen then results. Death can occur if the the dissection continues into the aortic valve causing severe aortic regurgitation or if the dissection ruptures into the pericardium causing cardiac tamponade. Other factors that increase mortality include obstruction of the abdominal aortic branch vessels causing end-organ failure or obstruction of the coronary artery causing myocardial infarction. Aortic dissections may be classified as acute or chronic. The acute phase is defined as the first two weeks, and during this time period, the risk of complications or aortic rupture is much higher compared to the chronic phase. Patients will commonly complain of symptoms in the early morning hours as this may be the time of day when the blood pressure is elevated. Chest or back pain is the most common presenting symptom. Patients with a prior history of diabetes or an aortic aneurysm may present with heart failure, syncope, or stroke symptoms. The pain associated with an aortic dissection usually begins abruptly and is severe and sharp in nature with radiation to the back. Weak pulses may occur secondary to impaired blood flow to the peripheral vessels. Often, patients may maintain a variation of over 20 mm Hg in systolic blood pressure between the arms. If the dissection involves the aortic valve, a diastolic murmur associated with aortic regurgitation may be appreciated at the right sternal border. Hypertension is more common in patients with descending aortic dissection compared to hypotension, which is a more classic presentation of ascending aortic dissections. An increase in heart rate of 120 beats per minute with standing (B) would likely be associated with postural orthostatic tachycardia syndrome (POTS). Tachycardia may occur as a compensatory mechanism to the hypotension associated with a dissection but it would not be impacted by position changes. Postural orthostatic tachycardia syndrome tends to be more common in teenage girls and will present with anxiety, palpitations, or dizziness. The auscultation of a carotid bruit (C) would classically correlate with carotid artery disease and occurs secondary to turbulent blood flow. It is not commonly associated with an aortic dissection, however, it can correlate with an increased risk of stroke. Chest pain that worsens with inspiration and improves with expiration (D) often correlates with a pulmonary embolism. This type of pain is referred to as pleuritic. While this symptom is not sensitive or specific for an aortic dissection, any patient with chest pain should be thoroughly evaluated for potential cardiac pathology. [/toggle]
[/accordion]
- Lee CC, Lee MT, Chen YS, et al. Risk of Aortic Dissection and Aortic Aneurysm in Patients Taking Oral Fluoroquinolone. JAMA Intern Med. 2015;175(11):1839-47.
- Lee CC, Lee MG, Hsieh R, et al. Oral Fluoroquinolone and the Risk of Aortic Dissection. J Am Coll Cardiol. 2018;72(12):1369-1378.
- Pasternak B, Inghammar M, Svanström H. Fluoroquinolone use and risk of aortic aneurysm and dissection: nationwide cohort study. BMJ. 2018;360:k678.
- Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients With Suspected Acute Nontraumatic Thoracic Aortic Dissection. Ann Emerg Med. 2015; 65(1)