We are in Berlin for #dasSMACC and have lots of pearls to share from the speakers at this amazing conference. Talks will be released for free on the SMACC podcast over the next year, but this podcast holds some pearls that we thought couldn’t wait.
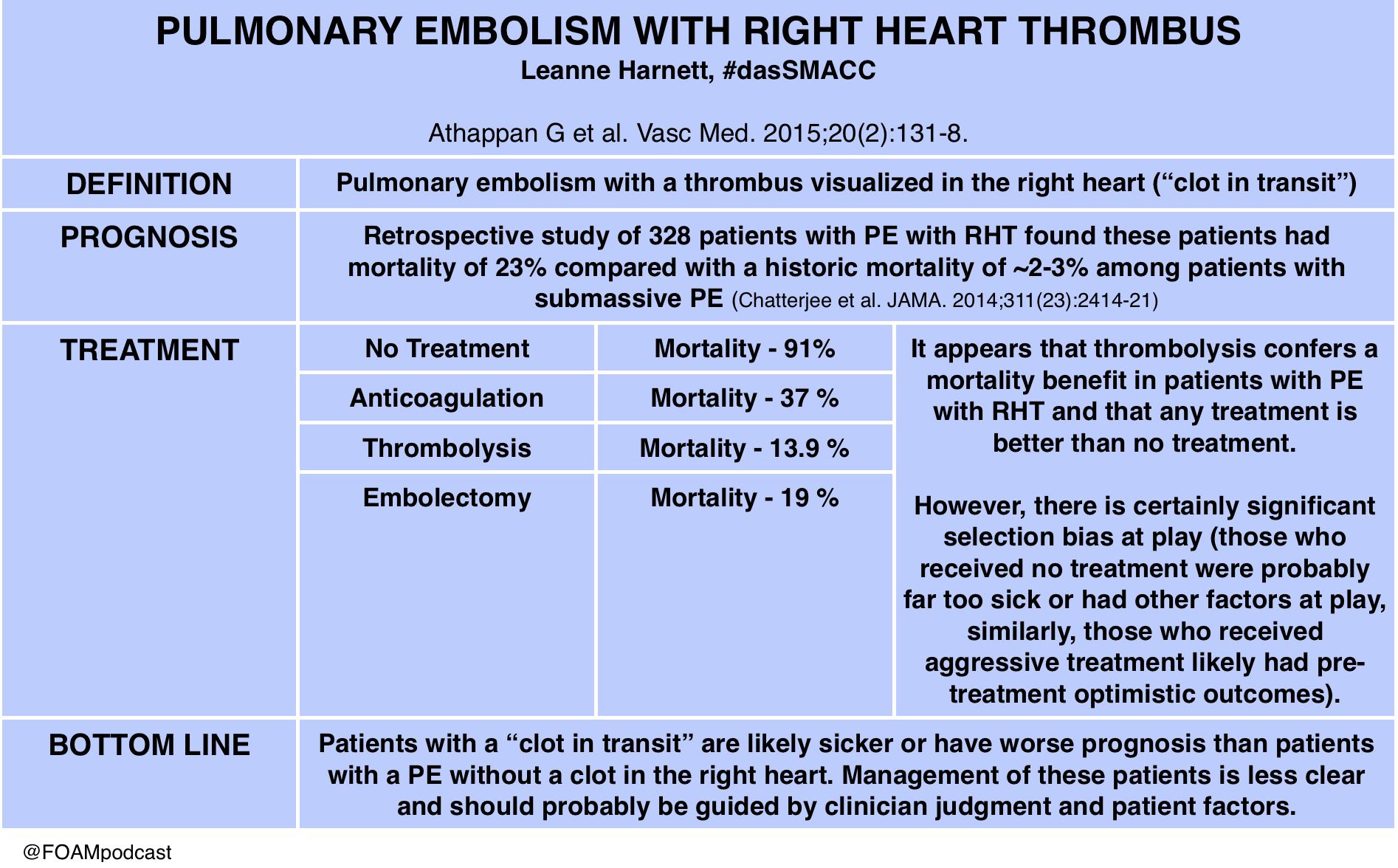
Dr. Leanne Harnett on Pulmonary Embolism with Right Heart Thrombus (PE with RHT)
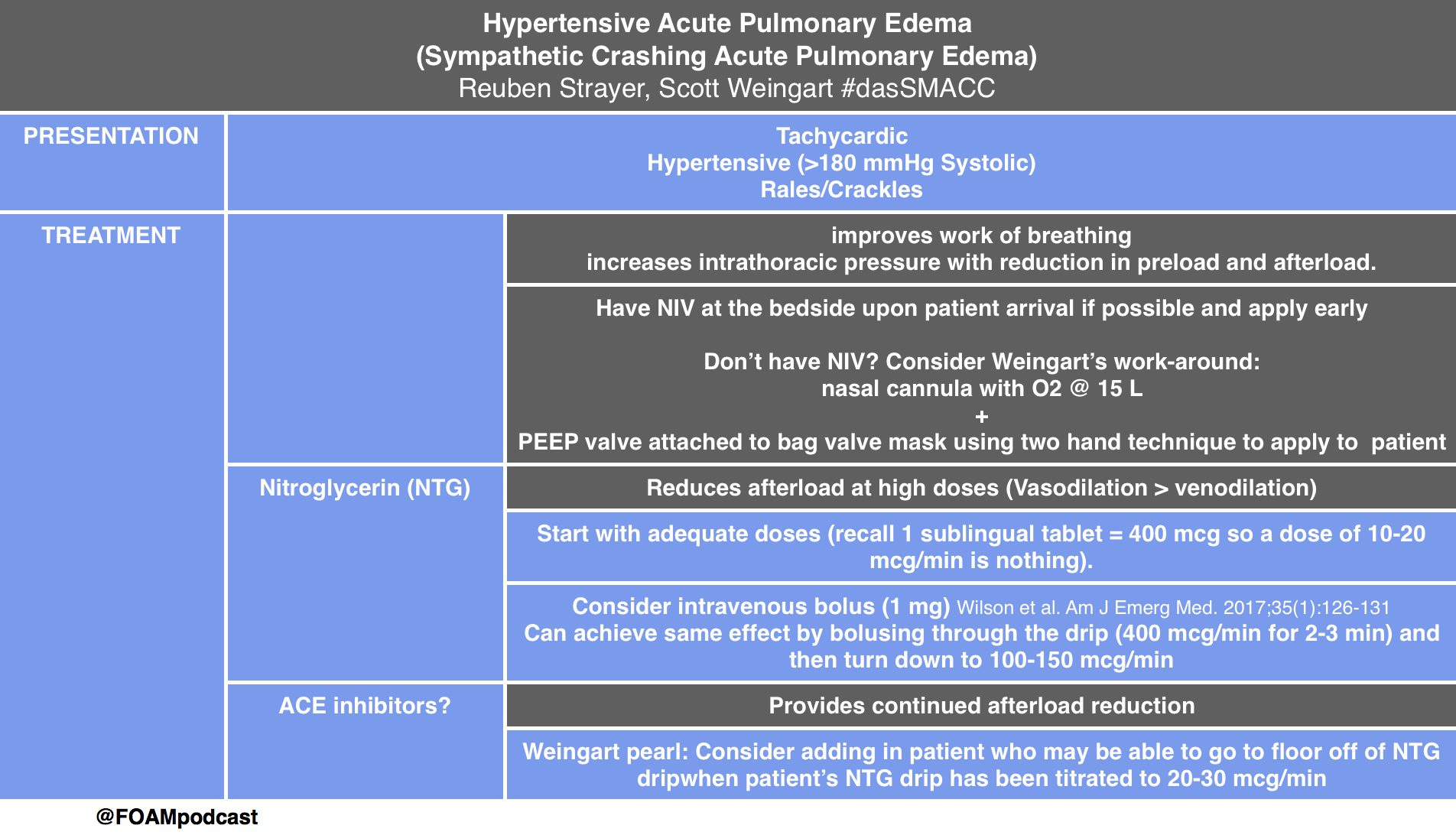
Drs. Reuben Strayer (@emupdates) and Scott Weingart (@emcrit) on Acute Hypertensive Pulmonary Edema
Dr. Michele Domico on Pediatric Cardiology Emergencies
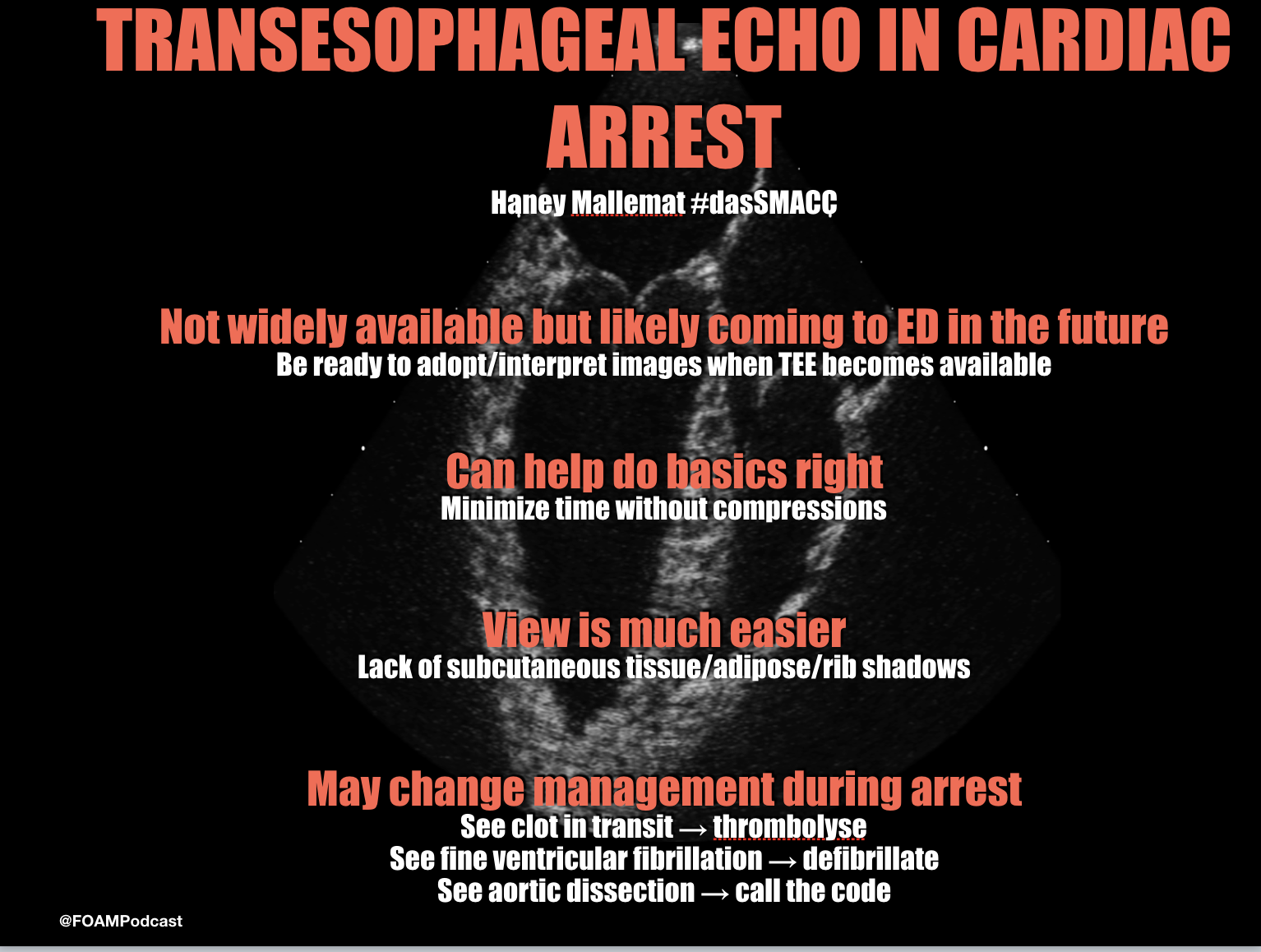
Dr. Haney Mallemat (@CriticalCareNow) on Transesophageal Echocardiography (TEE) during Cardiac Arrest
Athappan G, Sengodan P, Chacko P, Gandhi S. Comparative efficacy of different modalities for treatment of right heart thrombi in transit: a pooled analysis. Vasc Med. 2015;20(2):131-8.
Wilson SS, Kwiatkowski GM, Millis SR, Purakal JD, Mahajan AP, Levy PD. Use of nitroglycerin by bolus prevents intensive care unit admission in patients with acute hypertensive heart failure. Am J Emerg Med. 2017;35(1):126-131.
We are at #dasSMACC in Berlin thanks to the Rosh Review. All talks will be released for free on the SMACC podcast over the next year, but meanwhile, we wanted to share some pearls from the conference.
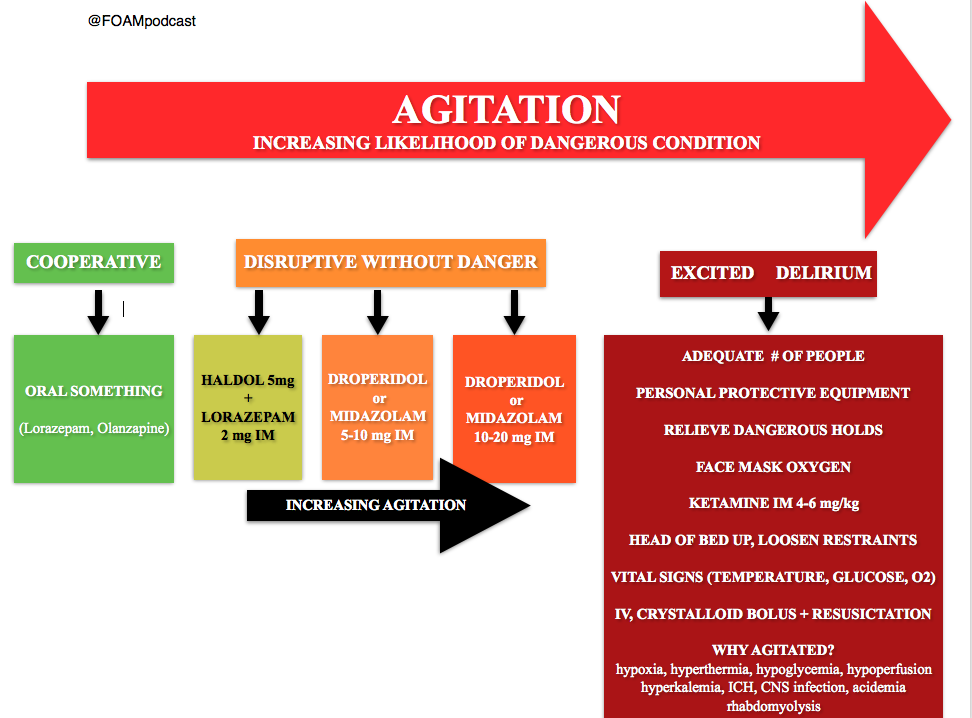
Dr. Reuben Strayer (@emupdates) – “Disruption, Danger, and Droperidol: Emergency Management of the Agitated Patient”
Dr. Strayer presented a brilliant talk on dealing with the quintessential Emergency Medicine patient – the undifferentiated acutely agitated patient. These patients are high risk and require emergent stabilization and resuscitation.
Dr. Reuben Strayer’s (@emupdates) algorithm for agitation in the ED
Oh, and, droperidol is not dangerous [1]. See this post on the controversial black box warning.
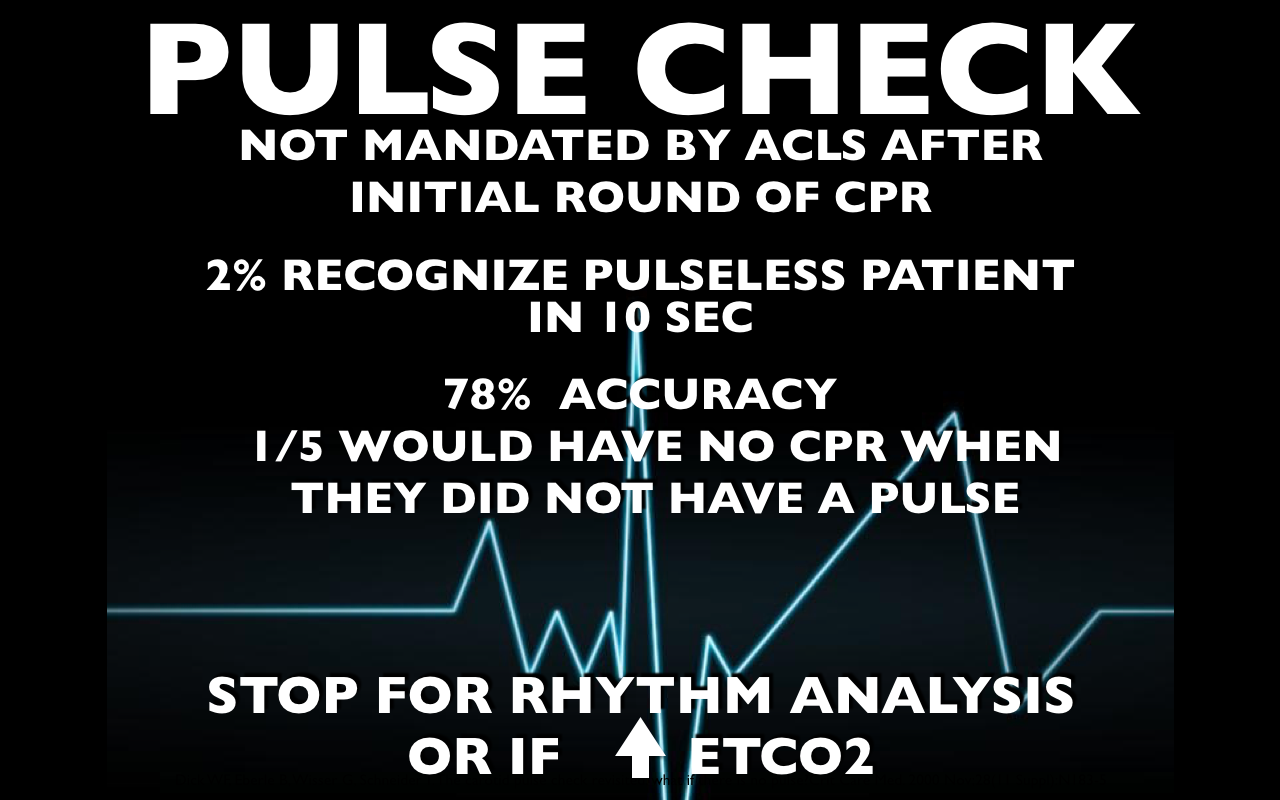
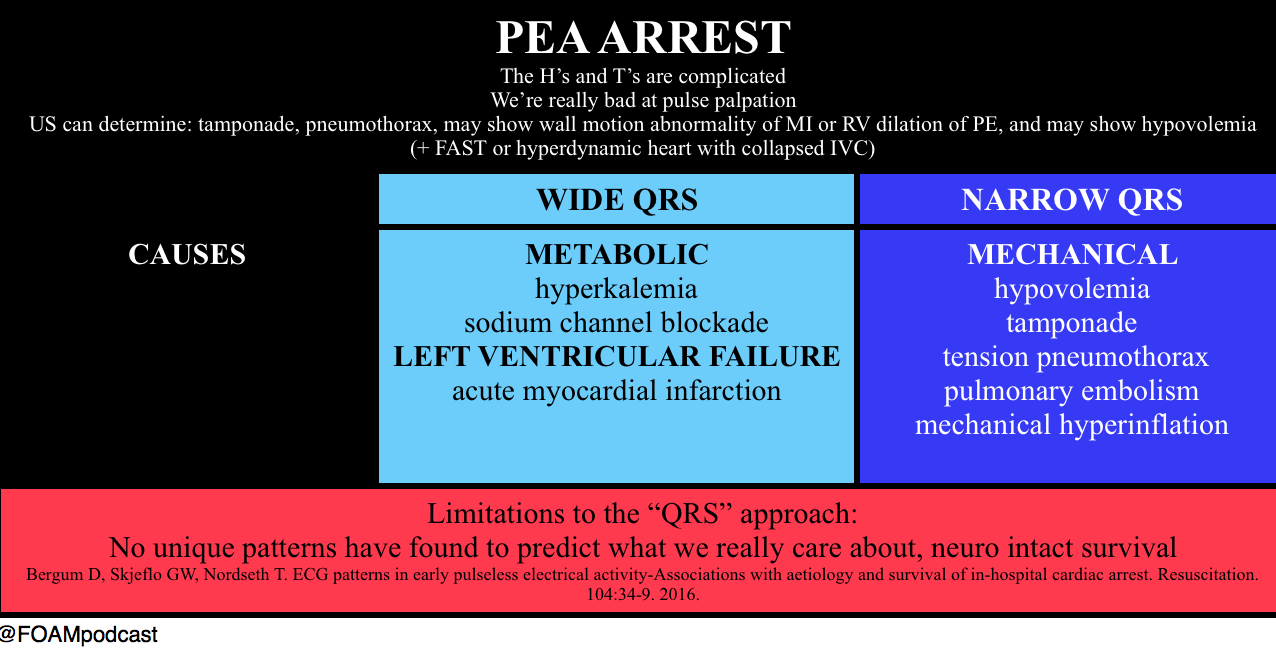
Dr. Haney Mallemat – “The PEA Paradox”
The typical way we think about PEA, the “H’s and T’s,” is overly complicated. Further, we are horrendous at pulse palpation (see this for more) [2,3], and so what we think is PEA may not actually be PEA. Dr. Mallemat proposed something along the lines of the following the following.
For some FOAM commentary on the limitations of this approach, see this post by Dr. Rory Spiegel [4].
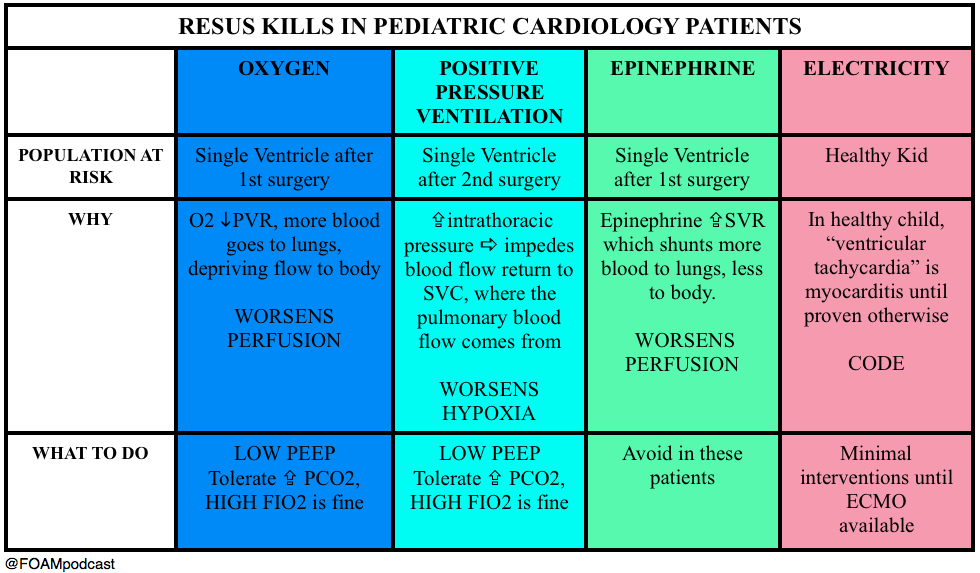
Dr. Michele Dominico – “How Usual Resuscitative Maneuvers Can Kill Paediatric Cardiac Patients”
Interventions we jump to in sick patients – oxygenation, ventilation, vasopressors – these can kill pediatric patients with cardiac pathology. She gave examples of some high yield pearls in these already terrifying patients.
EM Literature update by Drs. Ashley Shreves and Ryan Radecki
Ridiculous Research Pearls from Drs. Ashley Shreves and Ryan Radecki
Perception of dyspnea and pulmonary function tests change with stress – and rollercoaster rides. Rietveld S, van Beest I. Rollercoaster asthma: when positive emotional stress interferes with dyspnea perception. Behaviour research and therapy. 45(5):977-87. 2007. [pubmed]
Cured pork for epistaxis? Possibly.Researchers will try everything, especially if it involves bacon. Humphreys I, Saraiya S, Belenky W, Dworkin J. Nasal packing with strips of cured pork as treatment for uncontrollable epistaxis in a patient with Glanzmann thrombasthenia. The Annals of otology, rhinology, and laryngology. 120(11):732-6. 2011. [pubmed]
References:
Calver L, Page CB, Downes MA et al. The Safety and Effectiveness of Droperidol for Sedation of Acute Behavioral Disturbance in the Emergency Department. Annals of Emergency Medicine. 66(3):230-238.e1. 2015. [article]
Tibballs J, Weeranatna C. The influence of time on the accuracy of healthcare personnel to diagnose paediatric cardiac arrest by pulse palpation. Resuscitation. 81(6):671-5. 2010. [pubmed]
Eberle B, Dick WF, Schneider T, Wisser G, Doetsch S, Tzanova I. Checking the carotid pulse check: diagnostic accuracy of first responders in patients with and without a pulse. Resuscitation. 33(2):107-16. 1996. [pubmed]
FOAMcast will be back shortly with regular core content-cutting edge mash ups. However, we would be remiss not to take a moment to focus on a conference that inadvertently created FOAMcast…and is coming to Chicago in June 2015. SMACC – Chicago (#smaccUS) June 23-26, 2015.
The etiology: FOAMcast was dreamed up whilst milling around the exhibition hall at SMACC, discussing how even core content and “basic” medicine seemed cutting edge and important here. These projects can be dreamed up via Twitter or e-mail but I think there’s something special engendered by the propinquity of Free Open Access Medical education (FOAM) mixed with the physical conference. Our fate was sealed when Dr. Victoria Brazil happened to stop by to say “hi” while we were hyped up on “long blacks” and blabbering away about what we would call our project. For better or worse, FOAMcast was born.
Note: Please do not blame Dr. Brazil for our off-beat humor or the podcast. She had no idea what we were up to and does not endorse FOAMcast or Drs. Jeremy Faust and Lauren Westafer.
The talks at SMACC were unparalleled. The speakers inspiring, the slides clean, the material relevant, and the audience questions thoughtful. We learned from social workers (Liz Crowe’s hilarious talk), nurses, medics, and doctors from around the globe. In fact, we became friends, even the pre-med university student. We learned from them all.
The Core Content – There were a cornucopia of excellent core content talks; for example, Natalie May’s pediatric pearls, Aortic Catastrophes, and the Meaning of Acidosis by Dr. David Story. There are too many to list and they’re all worth a listen and can be found on iTunes or via the Intensive Care Network. Even the sonowars were brilliant. For example, Drs. Matt Dawson and Mike Mallin taught us to visualize cardiac view using humans. The awkward apical 4 chamber view for cardiac ultrasound:
Dr. Mallemat beautifully describes various methods of assessing fluid responsiveness – from IVC ultrasound (used alone, approximately equal to CVP), stroke volume variation, to passive leg raise and more advance ultrasound techniques.
Use dynamic markers rather than static numbers, which seemed to be universally lousy. Trend the patient’s response in order to give them “as much fluid as they need, and not one drop more.”
Source control is key in sepsis. If a patient has an infected gallbladder, obstructing kidney stone, etc – call surgery. Advocate for these patients.
ProCESS (and now ARISE) have demonstrated that protocols don’t necessarily have to be followed in order to reduce mortality in sepsis. We have become increasingly good at identifying and treating sepsis since the original EGDT trial. In his words – you don’t have to do sh*t, you just have to give a sh*t (Note: you still have to provide basic resuscitation, antibiotics, etc; you just don’t have to do the fancy stuff).
He had more pearls about lactate – such as in his collaborative, the number predicted badness but trends mattered less.
One cannot predict blood pressure based on the presence or absence of a pulse in various anatomic locales (i.e. if there’s a pulse at the radial artery, then their systolic blood pressure is at least >80 mmHg). This myth was taught for years and still persists in some trauma bays; however, even the evidence and the two most recent iterations of ATLS agree with Dr. Reid [Deakin et al]
Edema not solely due to hydrostatic pulmonary edema (i.e. should not be due to heart failure or fluid overload)
Bilateral infiltrates on CT/CXR *(subjective)
PaO2/FiO2 ratio <300 mmHg with at least 5 cm H20 of PEEP
The premise of Dr. Mac Sweeney’s talk; however, is that we ARDS is problematic because:
ARDS is a disease we can’t diagnose – Many of the criteria, although seemingly helped by the Berlin definition, are still subjective (ex: CXR Sensitivity 0.73; specificity, 0.70 [Figueroa-Casas]
The diagnosis of ARDS is of limited clinical utility. What he means by this is that the definition doesn’t really affect management and nearly all drugs targeted towards ARDS fail to show benefit consistently. The ARDS care that does work, like lung protective ventilation and fluid balance, these are just good critical care. Proning may work, but doesn’t seem to pan out in everyone [Guerin]. Dr. Mac Sweeney is also a little sweet on ECMO, awaiting future studies.
People don’t typically die from ARDS even though ARDS is associated with a 40-50% mortality rate. Yet, only 10% of people with ARDS die of ARDS or respiratory failure. Most people with ARDS die because they’re super sick.
Most people with ARDS don’t have ARDS. Autopsy studies have demonstrated that ~50% of people who met Berlin criteria for ARDS didn’t have the pathognomonic feature of ARDS, diffuse alveolar damage (DAD). The other half of the patients had pneumonia, abscesses, COPD, or other processes [Pinheiro et al, Thielle et al].
The crux of the ARDS issue per Dr. Mac Sweeney -It seems that ARDS is a fairly diverse spectrum with some subjectivity to the criteria. If approximately half of the people diagnosed with ARDS don’t have ARDS, then it’s no surprise that the therapies don’t benefit them. He leaves better identification in the hands of researchers.
In medicine we use teams or “tribes” to cope with stress, work together, and rally – Tribe Emergency Medicine, Tribe Anesthesiology, Tribe Surgery, etc. While making snarky comments, if in jest, may boost the morale and confidence of our team, this may be detrimental to overall patient care
SMACC – Built Friendships, Adventures, and Better Learners
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. Yesterday’s episode covered the council meetings.
Scientific Assembly Day 1 Pearls
Opening Session by Freakonomics hosts Steven Levitt and Stephen Dubner. Weird choice? It turns out that economists and physicians have a lot in common. What’s that? Probabilities. As physicians we like to think of ourselves as diagnosticians, but we’re more like probalisticians. We make predictions, hopefully based on the best evidence, our clinical expertise, and our patient’s values. People don’t remember the little stuff, like extra testing but they do tend to remember the more outlandish things, like the “amazing saves” or awful “misses.”
See this post by Dr. Simon Carley, in which he describes the ways in which physicians are really playing the odds and gambling.
Cardiology Pearls from Dr. Slovis.
Post cardiac arrest – targeted temperature management to 35-36 Celsius is the new 33 Celsius [Nielsen].
Many patients should probably go to the cath lab after arrest, but it’s still not clear exactly who benefits the most. STEMIs should probably go to the cath lab and, perhaps, non-STEMI ventricular fibrillation/tachycardia arrests. Apparently, 10-30% of these are actually STEMIs “on the inside” [More skeptical takes on this from Dr. Radecki here and here]
Infectious Disease Pearls from Dr. David Pigott – When someone returns from a developing nation, say, West Africa, the cause of their fever is not necessarily ebola. It’s probably an unknown, regular virus. It’s probably not ebola but it may be malaria which is quite common.
His thoughts on predictors of badness: Symptoms typically appear within 8-10 days although the “watch” period is 21 days. If a patient is in their second week of symptoms and are hemodynamically stable, then the patient has a pretty good shot.
Tox Pearls from Dr. Tim Erickson
Calcium channel blocker toxicity – you can try fluids, calcium, atropine, and vasopressors. For sick patients, however, insulin is the best bet (Note, FOAM is ahead of the curve: post on the lack of utility in glucagon from 2012).
Insulin bolus of 1 unit/kg followed by a drip of 1 unit/kg/h. Add dextrose at about 0.5 mg/kg/h, depending on their glucose.
Check glucose and potassium every 30 minutes, with the goal to keep the potassium 2.8-3.2, per Goldfrank.
Cyanide toxicity (discussed here) – if you’re thinking about it, please do NOT wait on a cyanide level, or any labs. Treat, with the current recommendation of intravenous hydroxocobalamin. There’s some discussion on the use of intramuscular cobinamide, which would be great in situations without IVs; however, this is largely untested in humans presently [Bebarta et al].
Dr. Scott Weingart – Catch the CO2 Wave (podcast). End tidal CO2 (ETCO2) – ETCO2 has become essential in monitoring patients in the ED. With anything we monitor, we really need to understand what we’re looking at as well as the interventions.
ETCO2 does NOT = PaCO2.
In most patients, the PaCO2 will be ~3-5 mmHg higher than their ETCO2.
This is because ETCO2 is really a measure of: PaCO2 (or production) but also cardiac output and alveolar ventilation. Thus, the ETCO2 may be falsely low in a patient with significant dead space, such as COPD, or with impaired cardiac output (heart failure).