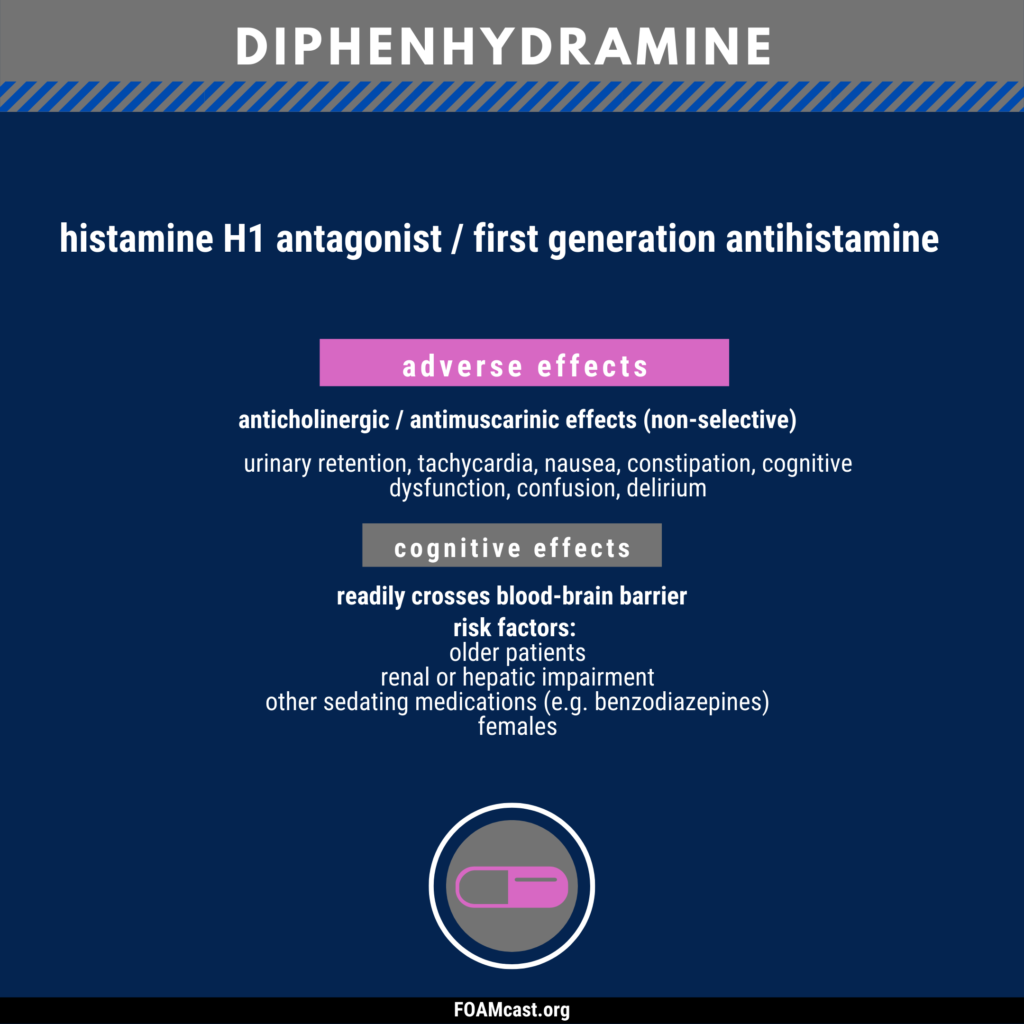
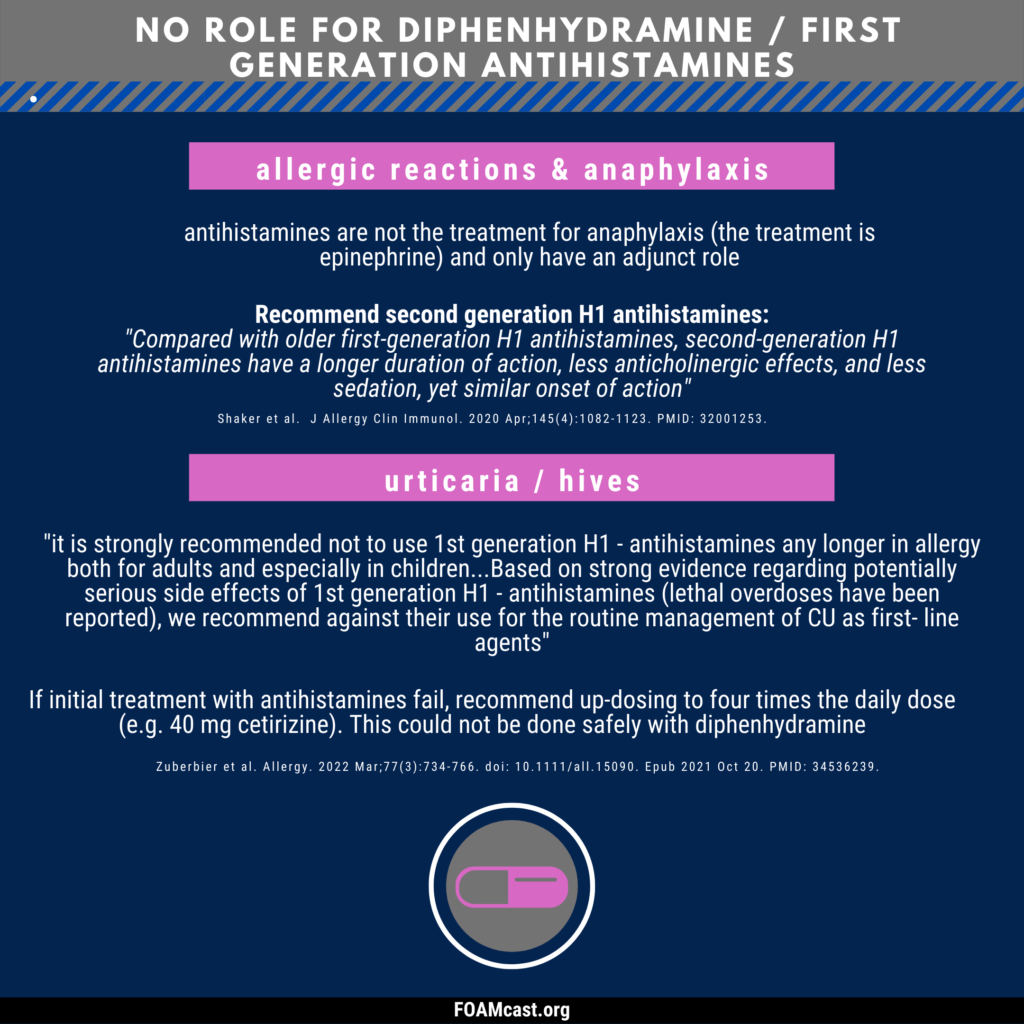
Diphenhydramine and other first-generation antihistamines are ubiquitous in medicine cabinets across the globe. Clinicians commonly recommend or administer diphenhydramine (Benadryl) for a variety of diseases – anaphylaxis, allergic reactions, urticaria, benign headaches/migraines, and as a sleep aid. However, professional societies have recommended against many of these indications for decades and, in other cases, there are safer alternatives. For more reading and references, see this article in ACEPnow.
We review Episode 1 of Dr. Salim Rezaie’s REBEL Cast covering exposing the dogma behind biphasic anaphylaxis reactions.
Traditionally, we’re taught to observe patients in the Emergency Department (ED) for 4-6 hours to watch out for biphasic reactions, as the rate of biphasic reactions can approach 20%.
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 27 ; Rosen’s 8(e) Chapter 119 but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Anaphylaxis
Diagnosis –
Two or more systems involved after likely allergen exposure (within hours):
Hypotension after exposure to known allergen for that patient (minutes to several hours)also qualifies
Differential Diagnosis -vasovagal (most common mimicker), myocardial ischemia, status asthmaticus, epiglottitis, angioedema, foreign body, carcinoid, vocal cord dysfunction, drug reactions, psychogenic
Treatment –
Epinephrine. Commit the dose to memory and look up if, needed as this is a huge source of medication errors [Gaeta et al, Benklefat ].
Adults: 0.3mg, Pediatrics 0.01mg/kg of 1:1000 epinephrine intramuscular (IM) to lateral thigh (pediatric patients >30kg get the adult dose).
If repeated doses of IM epinephrine required and patient continues to remain hypotensive, start intravenous epinephrine. ALiEM’s post on making the dirty epi drip.
Adjuncts:
IV fluids for blood pressure/shock
Corticosteroids may help prevent recurrence although they take 4-6 hours to work, so are unhelpful in acute attacks [Choo et al]. Rosen recommends either prednisone 0.5-1mg/kg orally or methylprednisolone 80-125 mg IV. (You don’t have to give IV in all cases)
Histamine blockers (H1 and H2 such as diphenhydramine and famotidine, respectively) may help with the dermatologic symptoms and pruritis.
Glucagon in patients that aren’t responding or are on beta-blockers. ALiEM post.
Give patients that are going home a prescription for an EpiPen (for pediatric patients, have one parent go fill the script during the observation period) and show them how to use the autoinjector. These things are expensive and do expire, and there are some coupons out there to help out.
Disposition – Clearly patients with ongoing symptoms and/or shock should stay in the hospital. However, most patients can be discharged home once they are improved and the effects of the epinephrine have worn off. Tintinalli recommends about 4 hours, referencing a study by Brady et al from 2007. Interestingly, in this study there were 2 biphasic reactions that occurred at 20 hours and 46 hours after the initial ED visit. So, not sure how they came up with 4 hours.
FOAM Pearls Supported by the Literature and Rosenalli –
Shellfish allergy does NOT put a patient at increased risk of contrast allergy more than any other allergen [Kaufman et al].
Cross-reactivity between penicillin and cephalosporins is often quoted at 10-20% but, in reality, is far less and a review demonstrates cross reactivity of 1% in patients reporting a penicillin allergy [Campagna et al]. Rosen’s agrees with this assessment and states that the overall cross reactivity is minimal. ALiEM post on this myth
ACE-Inhibitor Induced Angioedema
Cause: The vasodilation and non-pitting edema of the mucosal, dermal, and subcutaneous tissues thought to be mediated by the build up of bradykinin and substance P. Non-allergic, often asymmetric.
Presentation: Swelling of the lips, tongue, airway most often although it can also involve the genitals and viscera.
Epinephrine, corticosteroids, and histamine blockers do not work. While fresh frozen plasma may work for hereditary angioedema, but it doesn’t really work in ACE-inhibitor angioedema and there’s no proven therapy [Winters et al].
Investigations underway for icatibant (bradykinin 2 receptor antagonist) Bas et al, Schmidt et al and Ecallantide (reversible kallikrein inhibitor)
Question 1. A 55-year old man who is taking several antihypertensive medications presents to the ED with nausea, vomiting, shortness of breath, and a rash after eating a home-cooked Thai meal at a friend’s house about 1 hour ago. The symptoms began within seconds of the first bite of his meal. Despite the patient being administered 2 doses of intramuscular epinephrine, diphenhydramine, dexamethasone, and crystalloid fluids, his blood pressure remains at 75/38 mm Hg.Which other medication should be considered in this patient?
A. Cimetidine
B. Glucagon
C. Norepinephrine
D. Octreotide
Question 2. A 55-year-old woman presents to the ED for swelling of her tongue and lips.
Photo: Rosh Review
She recently started a new antihypertensive medication. Which of the following is the direct mediator for her condition?
A. Angiotensin
B. Bradykinin
C. C1-esterase inhibitor
D. Histamine
Answers.
1. B. The patient is experiencing an acute anaphylactic reaction, most likely to peanuts that are commonly found in Thai cooking. Although uncommon, patients taking beta-blocking agents for hypertension may exhibit refractory hypotension despite being administered fluids and epinephrine. This is because epinephrine acts by binding to adrenergic receptors, which includes beta-receptors. To circumvent the beta-receptor, glucagon can be administered, which will bypass the beta-adrenergic second messenger system, potentiate the circulating epinephrine, and help restore vasomotor tone.
Cimetidine (A) is an antihistamine. Although it may help in mild allergic reactions, it will not treat hypotension in severe anaphylaxis. In addition, cimetidine prolongs the metabolism of beta-blockers. Octreotide (D) may be used in management of esophageal variceal bleeding control, treatment of carcinoid syndrome, and refractory hypoglycemia after sulfonylurea-induced hypoglycemia. There is no role in anaphylaxis. Norepinephrine (C) also binds adrenergic receptors that may be inhibited in patients who take beta-blocking medications.
2. B. Angioedema is the clinical manifestation of transient, localized, nonpitting swelling of the subcutaneous layer of the skin or submucosal layer of the respiratory or gastrointestinal tracts. There are many cases of angioedema, but the condition is usually divided into hereditary, acquired, and drug-induced causes. Hereditary angioedema (HAE) is caused by deficiency or dysfunction of C1-esterase inhibitor and is usually precipitated by stress or trauma. Acquired angioedema is also due to deficiency or dysfunction of C1-esterase inhibitor, but is not due to a genetic cause; rather, it appears later in life. The exact etiology is unknown, but the condition is exceedingly rare. The most common cause of drug-induced angioedema is due to an adverse reaction from ACE inhibitors. When ACE is inhibited by medications, angiotensin I is not converted to angiotensin II, and bradykinin is not metabolized. It is thought that the increased level of bradykinin is responsible for angioedema induced by ACE inhibitors. Angioedema can result in severe airway compromise or, less commonly, compromise in the GI tract that is associated with abdominal pain. Evaluation should focus on ruling out laryngeal edema and airway compromise. Although direct visualization is best, asking the patient to phonate a high-pitched “E” is one quick way of assessing for laryngeal edema. If the patient is able to phonate a high-pitched “E,” then the presence of laryngeal edema is unlikely. Treatment is mainly supportive with special attention to airway protection. Angioedema caused by deficiency or dysfunction of C1-esterase inhibitor can be treated by replacing C1-esterase inhibitor with fresh frozen plasma or other recombinant agents.
Angiotensin (A) is a peptide hormone that causes vasoconstriction and a subsequent increase in blood pressure. It is part of the renin-angiotensin system, which is a major target for drugs (ACE inhibitors) that lower blood pressure. An elevated level of angiotensin is not responsible for angioedema. C1-esterase inhibitor (C) serves as the main regulator of the kallikrein-kinin system. As a result of decreased amounts of functional C1-INH, when the kallikrein-kinin system is activated, it is not kept in check. This leads to increased formation of bradykinin and the resultant increased vascular permeability and edema formation and is the cause of hereditary angioedema, not ACE-inhibitor induced angioedema. Histamine (D) has many roles in the body, but its primary role is within the immune system. Mast cells release histamine through a process known as degranulation when they have been sensitized with IgE antibodies and then come in contact with an appropriate antigen leading to the development of urticaria and pruritus.
We review Episode 1 of Dr. Salim Rezaie’s REBEL Cast covering exposing the dogma behind biphasic anaphylaxis reactions.
Traditionally, we’re taught to observe patients in the Emergency Department (ED) for 4-6 hours to watch out for biphasic reactions, as the rate of biphasic reactions can approach 20%.
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 27 ; Rosen’s 8(e) Chapter 119 but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Anaphylaxis
Diagnosis –
Two or more systems involved after likely allergen exposure (within hours):
Hypotension after exposure to known allergen for that patient (minutes to several hours)also qualifies
Differential Diagnosis -vasovagal (most common mimicker), myocardial ischemia, status asthmaticus, epiglottitis, angioedema, foreign body, carcinoid, vocal cord dysfunction, drug reactions, psychogenic
Treatment –
Epinephrine. Commit the dose to memory and look up if, needed as this is a huge source of medication errors [Gaeta et al, Benklefat ].
Adults: 0.3mg, Pediatrics 0.01mg/kg of 1:1000 epinephrine intramuscular (IM) to lateral thigh (pediatric patients >30kg get the adult dose).
If repeated doses of IM epinephrine required and patient continues to remain hypotensive, start intravenous epinephrine. ALiEM’s post on making the dirty epi drip.
Adjuncts:
IV fluids for blood pressure/shock
Corticosteroids may help prevent recurrence although they take 4-6 hours to work, so are unhelpful in acute attacks [Choo et al]. Rosen recommends either prednisone 0.5-1mg/kg orally or methylprednisolone 80-125 mg IV. (You don’t have to give IV in all cases)
Histamine blockers (H1 and H2 such as diphenhydramine and famotidine, respectively) may help with the dermatologic symptoms and pruritis.
Glucagon in patients that aren’t responding or are on beta-blockers. ALiEM post.
Give patients that are going home a prescription for an EpiPen (for pediatric patients, have one parent go fill the script during the observation period) and show them how to use the autoinjector. These things are expensive and do expire, and there are some coupons out there to help out.
Disposition – Clearly patients with ongoing symptoms and/or shock should stay in the hospital. However, most patients can be discharged home once they are improved and the effects of the epinephrine have worn off. Tintinalli recommends about 4 hours, referencing a study by Brady et al from 2007. Interestingly, in this study there were 2 biphasic reactions that occurred at 20 hours and 46 hours after the initial ED visit. So, not sure how they came up with 4 hours.
FOAM Pearls Supported by the Literature and Rosenalli –
Shellfish allergy does NOT put a patient at increased risk of contrast allergy more than any other allergen [Kaufman et al].
Cross-reactivity between penicillin and cephalosporins is often quoted at 10-20% but, in reality, is far less and a review demonstrates cross reactivity of 1% in patients reporting a penicillin allergy [Campagna et al]. Rosen’s agrees with this assessment and states that the overall cross reactivity is minimal. ALiEM post on this myth
ACE-Inhibitor Induced Angioedema
Cause: The vasodilation and non-pitting edema of the mucosal, dermal, and subcutaneous tissues thought to be mediated by the build up of bradykinin and substance P. Non-allergic, often asymmetric.
Presentation: Swelling of the lips, tongue, airway most often although it can also involve the genitals and viscera.
Epinephrine, corticosteroids, and histamine blockers do not work. While fresh frozen plasma may work for hereditary angioedema, but it doesn’t really work in ACE-inhibitor angioedema and there’s no proven therapy [Winters et al].
Investigations underway for icatibant (bradykinin 2 receptor antagonist) Bas et al, Schmidt et al and Ecallantide (reversible kallikrein inhibitor)
Question 1. A 55-year old man who is taking several antihypertensive medications presents to the ED with nausea, vomiting, shortness of breath, and a rash after eating a home-cooked Thai meal at a friend’s house about 1 hour ago. The symptoms began within seconds of the first bite of his meal. Despite the patient being administered 2 doses of intramuscular epinephrine, diphenhydramine, dexamethasone, and crystalloid fluids, his blood pressure remains at 75/38 mm Hg.Which other medication should be considered in this patient?
A. Cimetidine
B. Glucagon
C. Norepinephrine
D. Octreotide
Question 2. A 55-year-old woman presents to the ED for swelling of her tongue and lips.
Photo: Rosh Review
She recently started a new antihypertensive medication. Which of the following is the direct mediator for her condition?
A. Angiotensin
B. Bradykinin
C. C1-esterase inhibitor
D. Histamine
Answers.
1. B. The patient is experiencing an acute anaphylactic reaction, most likely to peanuts that are commonly found in Thai cooking. Although uncommon, patients taking beta-blocking agents for hypertension may exhibit refractory hypotension despite being administered fluids and epinephrine. This is because epinephrine acts by binding to adrenergic receptors, which includes beta-receptors. To circumvent the beta-receptor, glucagon can be administered, which will bypass the beta-adrenergic second messenger system, potentiate the circulating epinephrine, and help restore vasomotor tone.
Cimetidine (A) is an antihistamine. Although it may help in mild allergic reactions, it will not treat hypotension in severe anaphylaxis. In addition, cimetidine prolongs the metabolism of beta-blockers. Octreotide (D) may be used in management of esophageal variceal bleeding control, treatment of carcinoid syndrome, and refractory hypoglycemia after sulfonylurea-induced hypoglycemia. There is no role in anaphylaxis. Norepinephrine (C) also binds adrenergic receptors that may be inhibited in patients who take beta-blocking medications.
2. B. Angioedema is the clinical manifestation of transient, localized, nonpitting swelling of the subcutaneous layer of the skin or submucosal layer of the respiratory or gastrointestinal tracts. There are many cases of angioedema, but the condition is usually divided into hereditary, acquired, and drug-induced causes. Hereditary angioedema (HAE) is caused by deficiency or dysfunction of C1-esterase inhibitor and is usually precipitated by stress or trauma. Acquired angioedema is also due to deficiency or dysfunction of C1-esterase inhibitor, but is not due to a genetic cause; rather, it appears later in life. The exact etiology is unknown, but the condition is exceedingly rare. The most common cause of drug-induced angioedema is due to an adverse reaction from ACE inhibitors. When ACE is inhibited by medications, angiotensin I is not converted to angiotensin II, and bradykinin is not metabolized. It is thought that the increased level of bradykinin is responsible for angioedema induced by ACE inhibitors. Angioedema can result in severe airway compromise or, less commonly, compromise in the GI tract that is associated with abdominal pain. Evaluation should focus on ruling out laryngeal edema and airway compromise. Although direct visualization is best, asking the patient to phonate a high-pitched “E” is one quick way of assessing for laryngeal edema. If the patient is able to phonate a high-pitched “E,” then the presence of laryngeal edema is unlikely. Treatment is mainly supportive with special attention to airway protection. Angioedema caused by deficiency or dysfunction of C1-esterase inhibitor can be treated by replacing C1-esterase inhibitor with fresh frozen plasma or other recombinant agents.
Angiotensin (A) is a peptide hormone that causes vasoconstriction and a subsequent increase in blood pressure. It is part of the renin-angiotensin system, which is a major target for drugs (ACE inhibitors) that lower blood pressure. An elevated level of angiotensin is not responsible for angioedema. C1-esterase inhibitor (C) serves as the main regulator of the kallikrein-kinin system. As a result of decreased amounts of functional C1-INH, when the kallikrein-kinin system is activated, it is not kept in check. This leads to increased formation of bradykinin and the resultant increased vascular permeability and edema formation and is the cause of hereditary angioedema, not ACE-inhibitor induced angioedema. Histamine (D) has many roles in the body, but its primary role is within the immune system. Mast cells release histamine through a process known as degranulation when they have been sensitized with IgE antibodies and then come in contact with an appropriate antigen leading to the development of urticaria and pruritus.