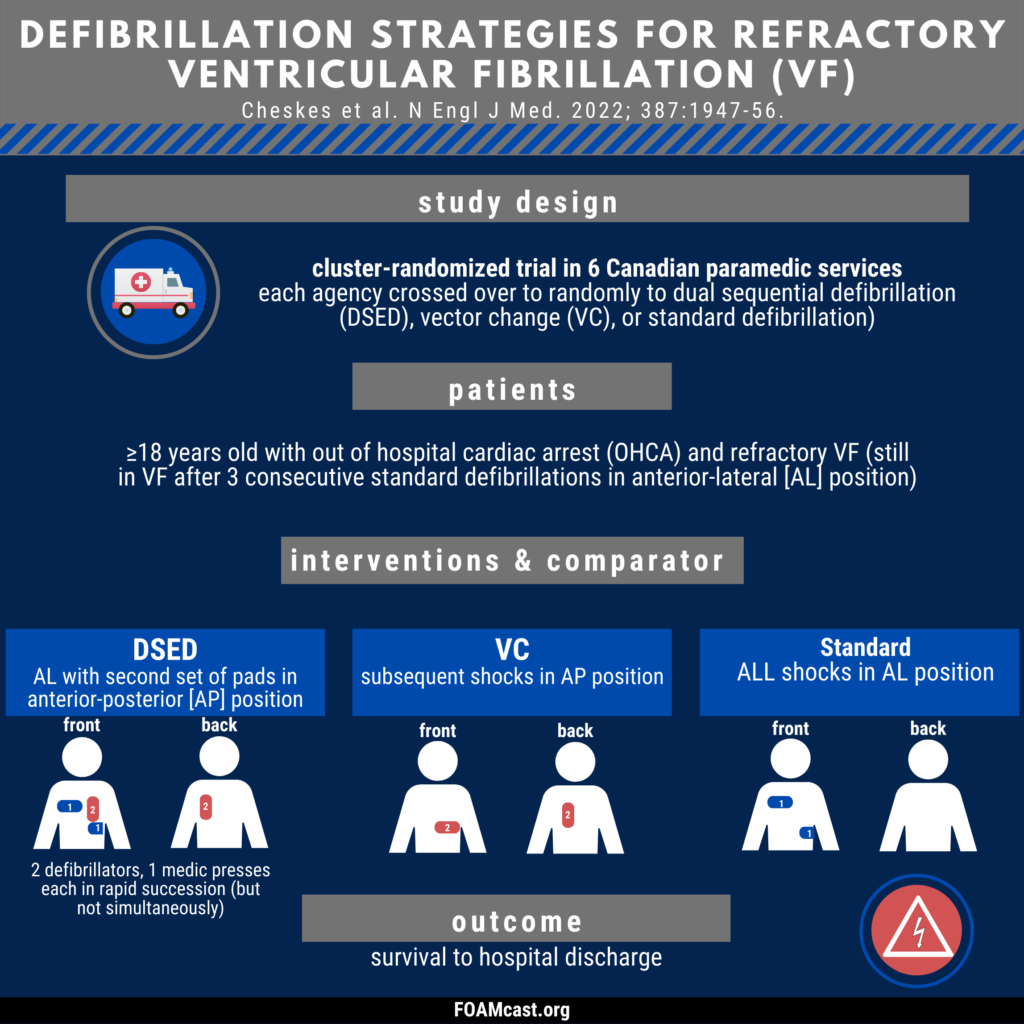
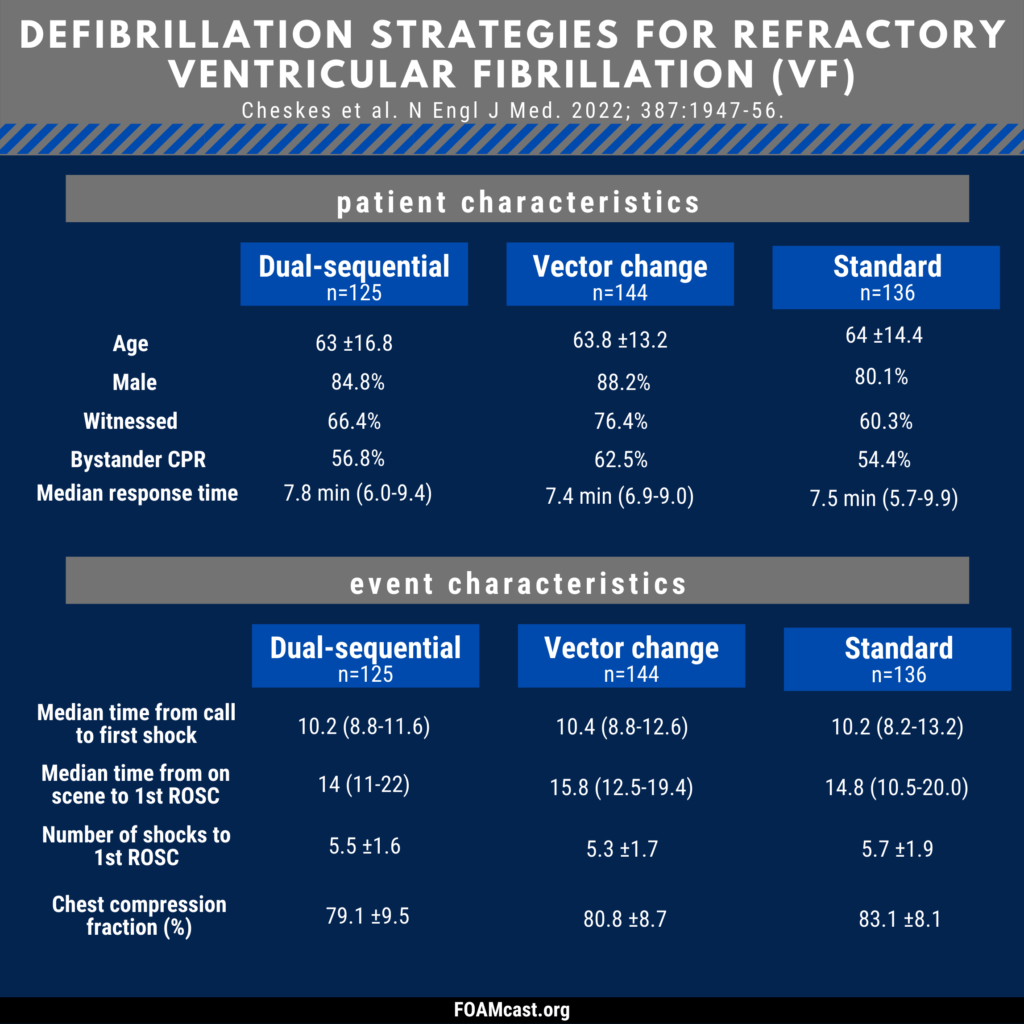
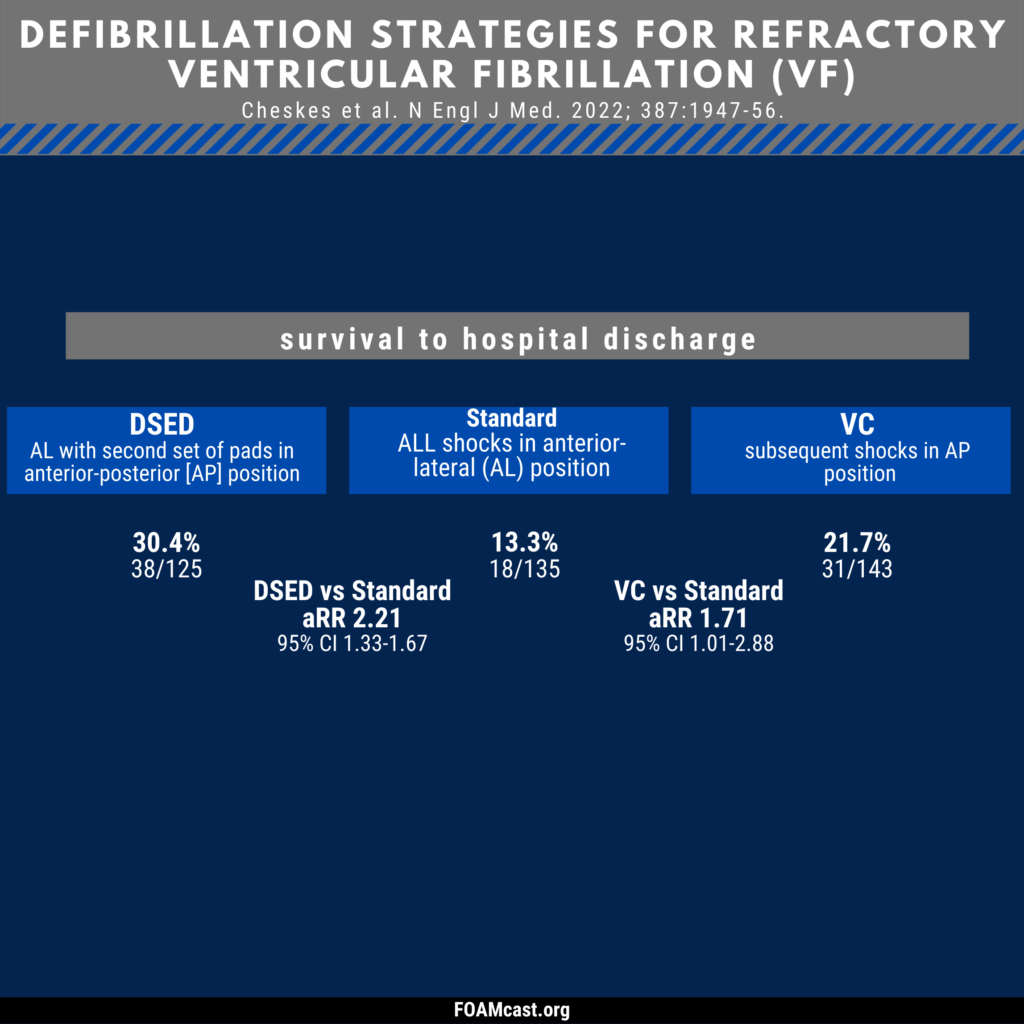
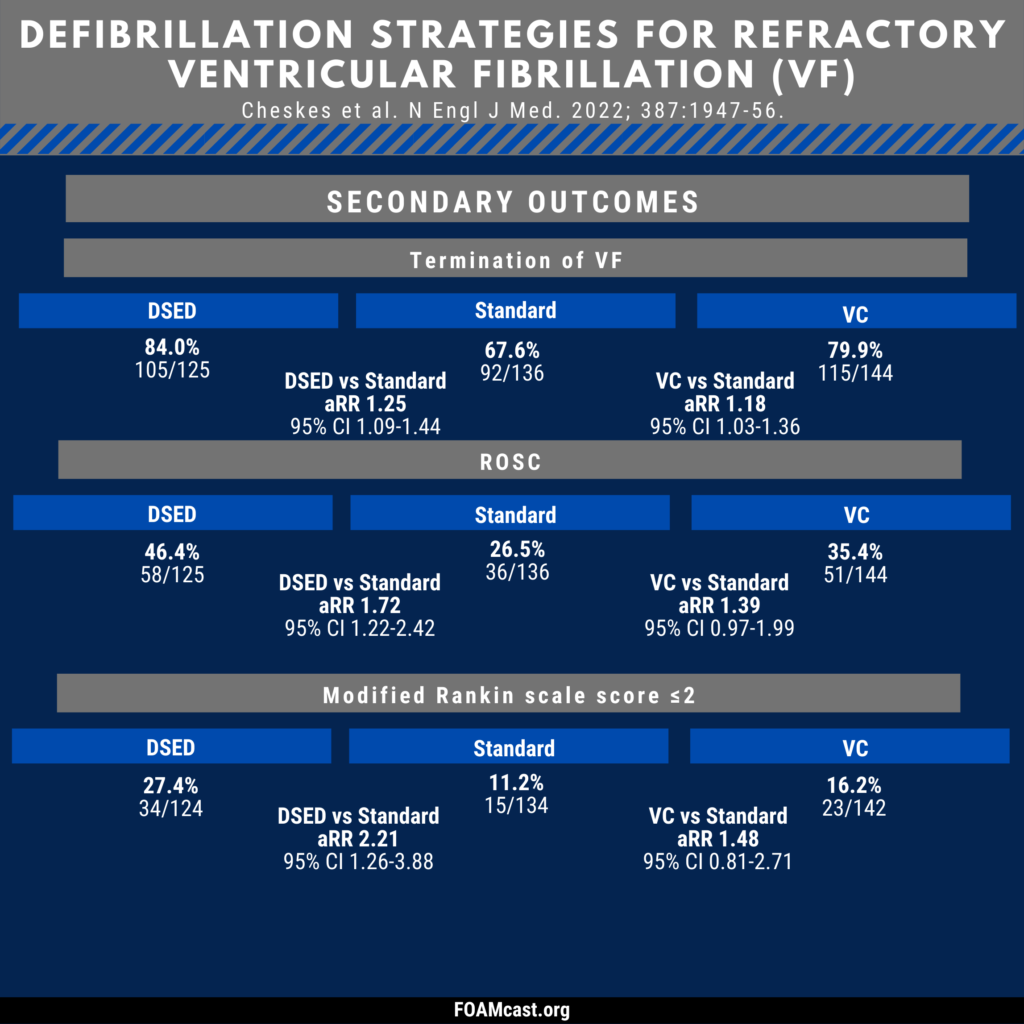
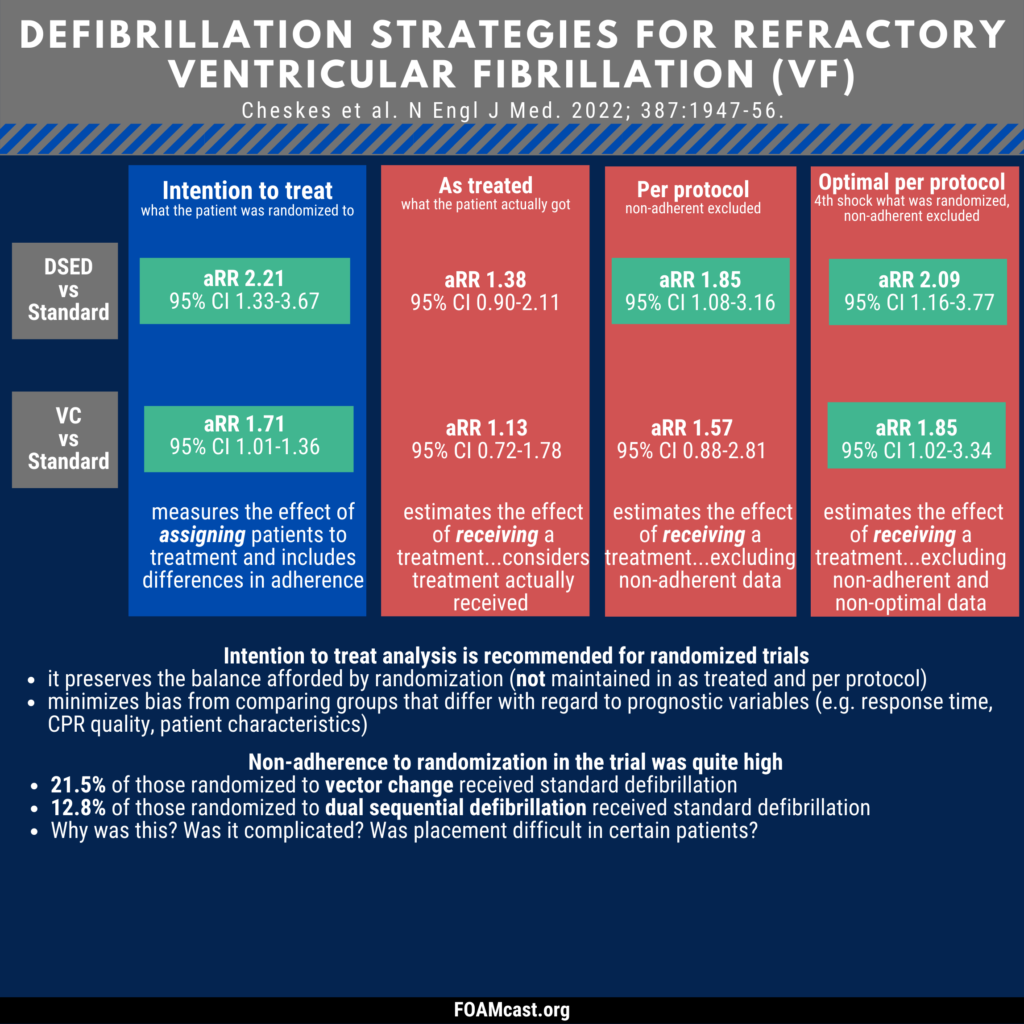
In this episode, we review the largest trial of double sequential external defibrillation (DSED) and vector change (VC) defibrillation for refractory ventricular fibrillation (VFib): Cheskes S, Verbeek PR, Drennan IR, et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022;387(21):1947-1956.
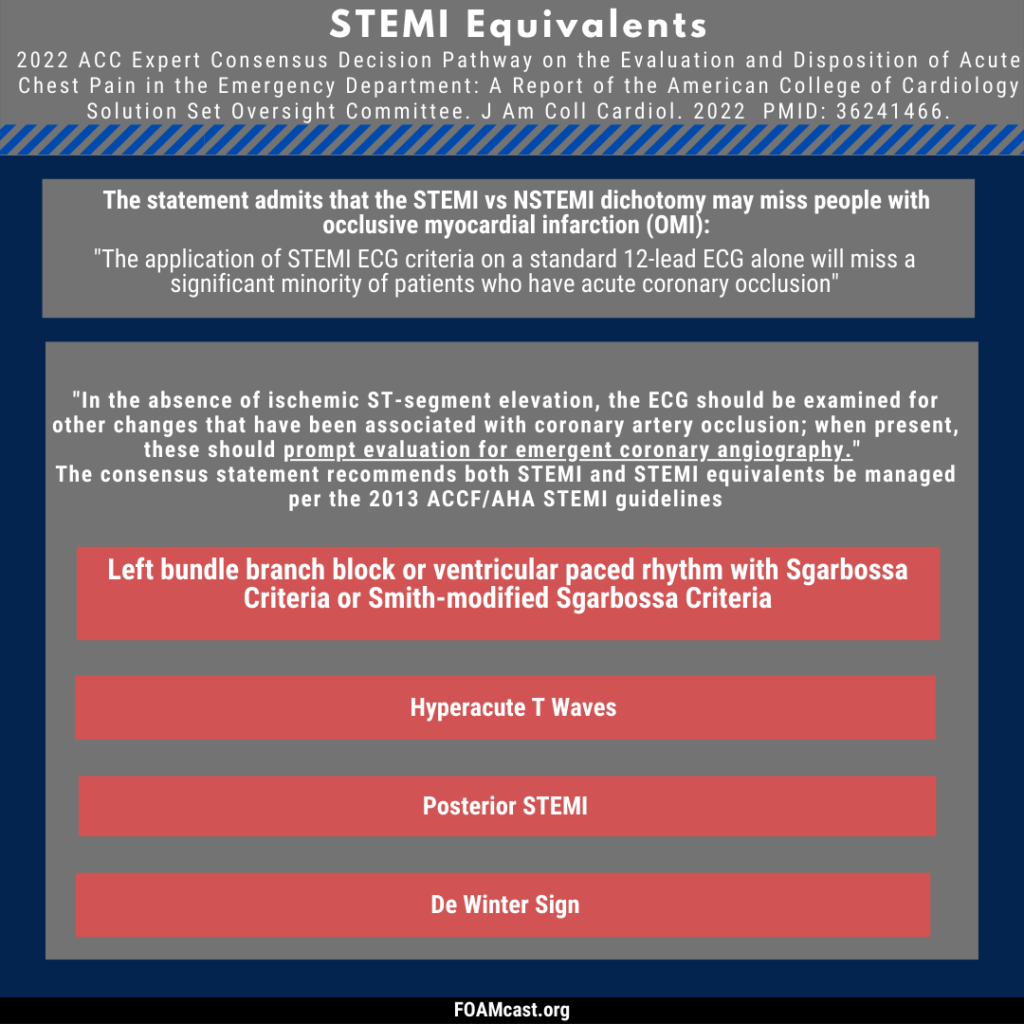
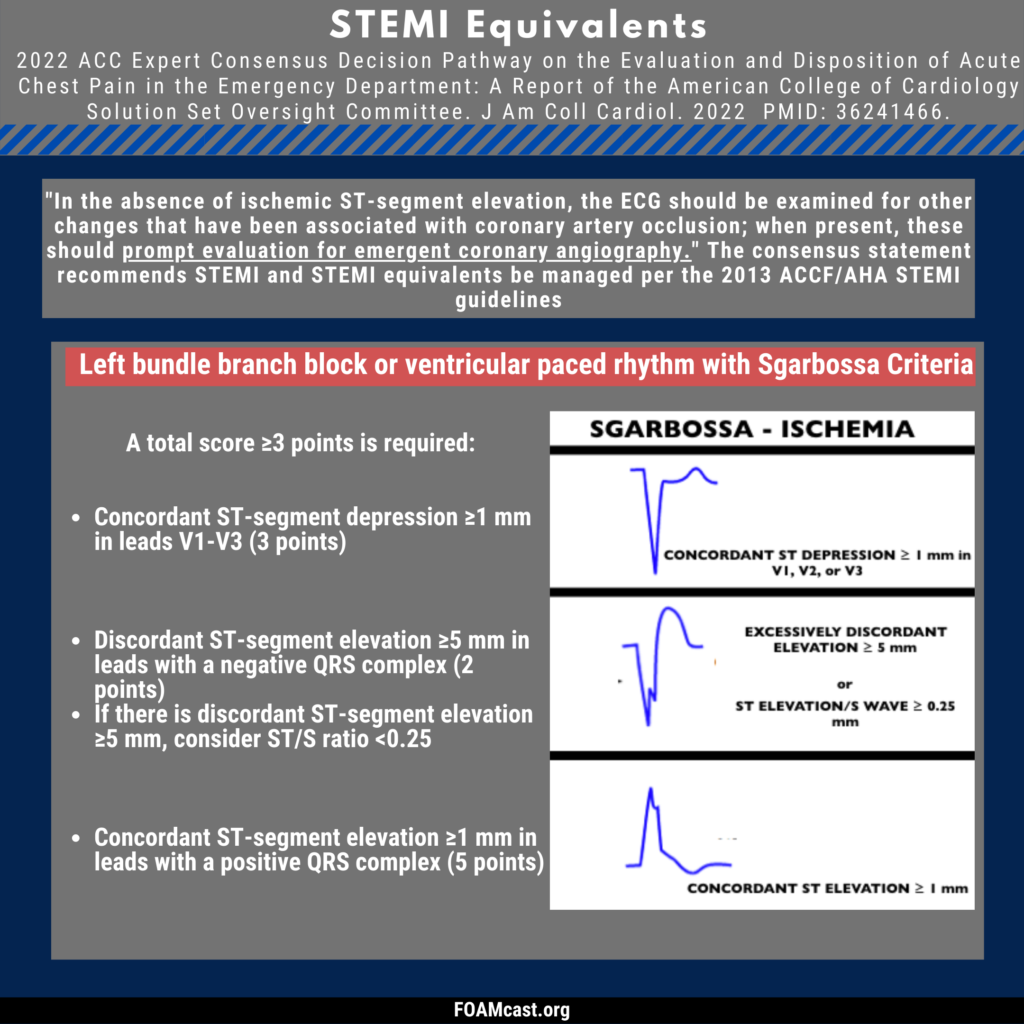
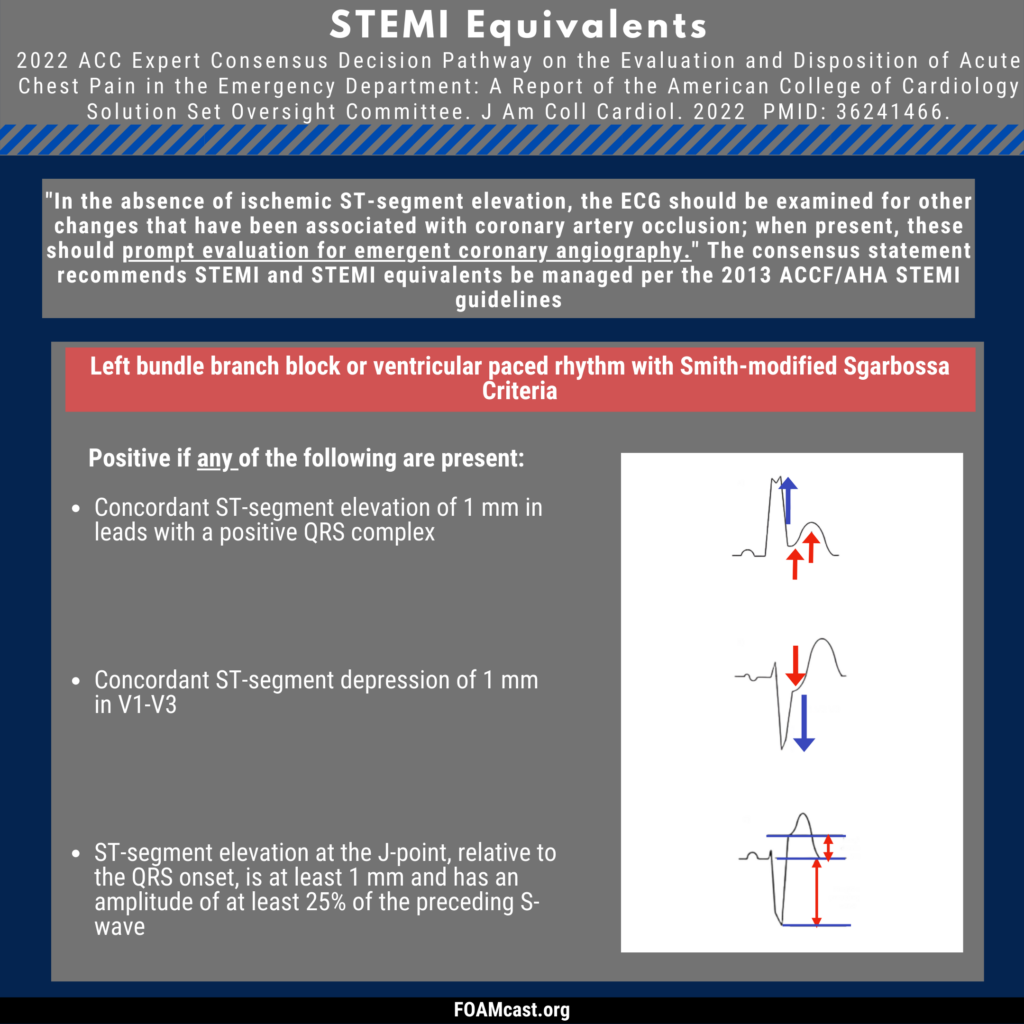
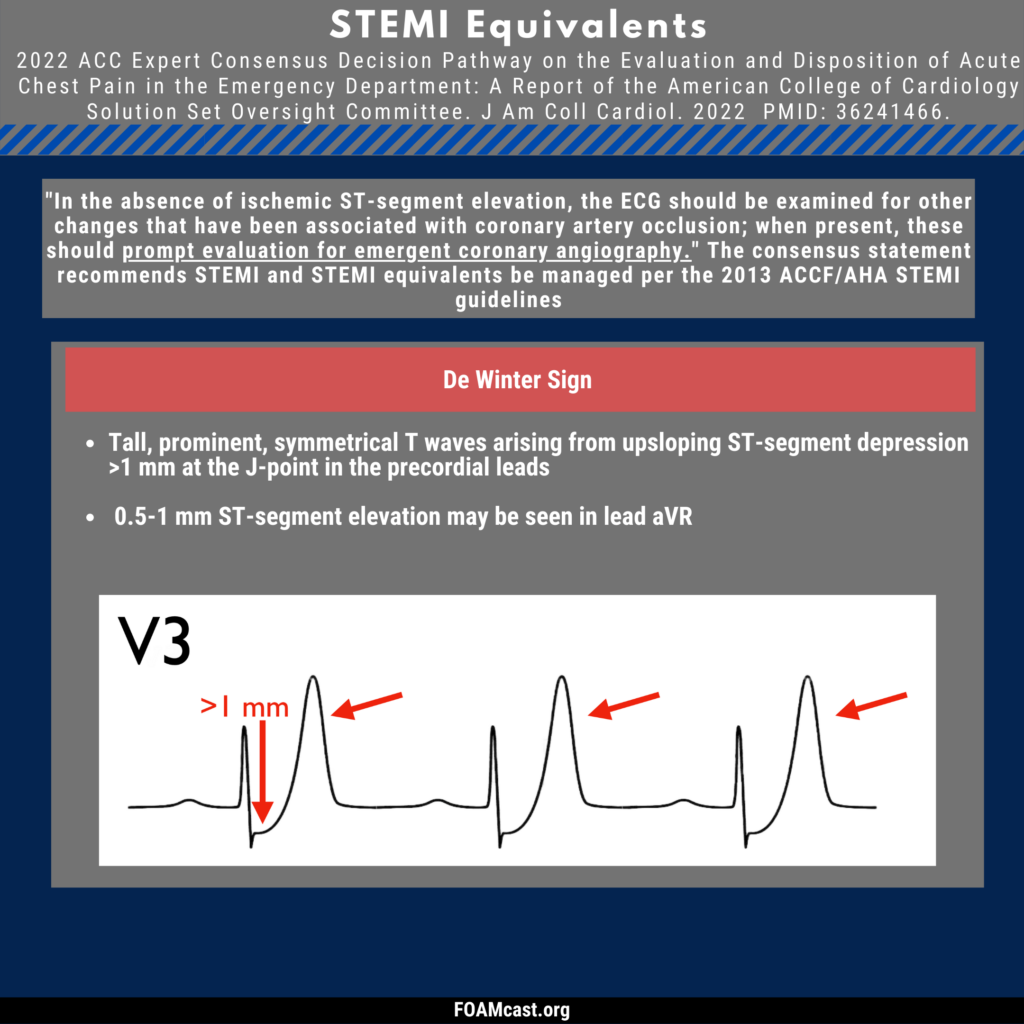
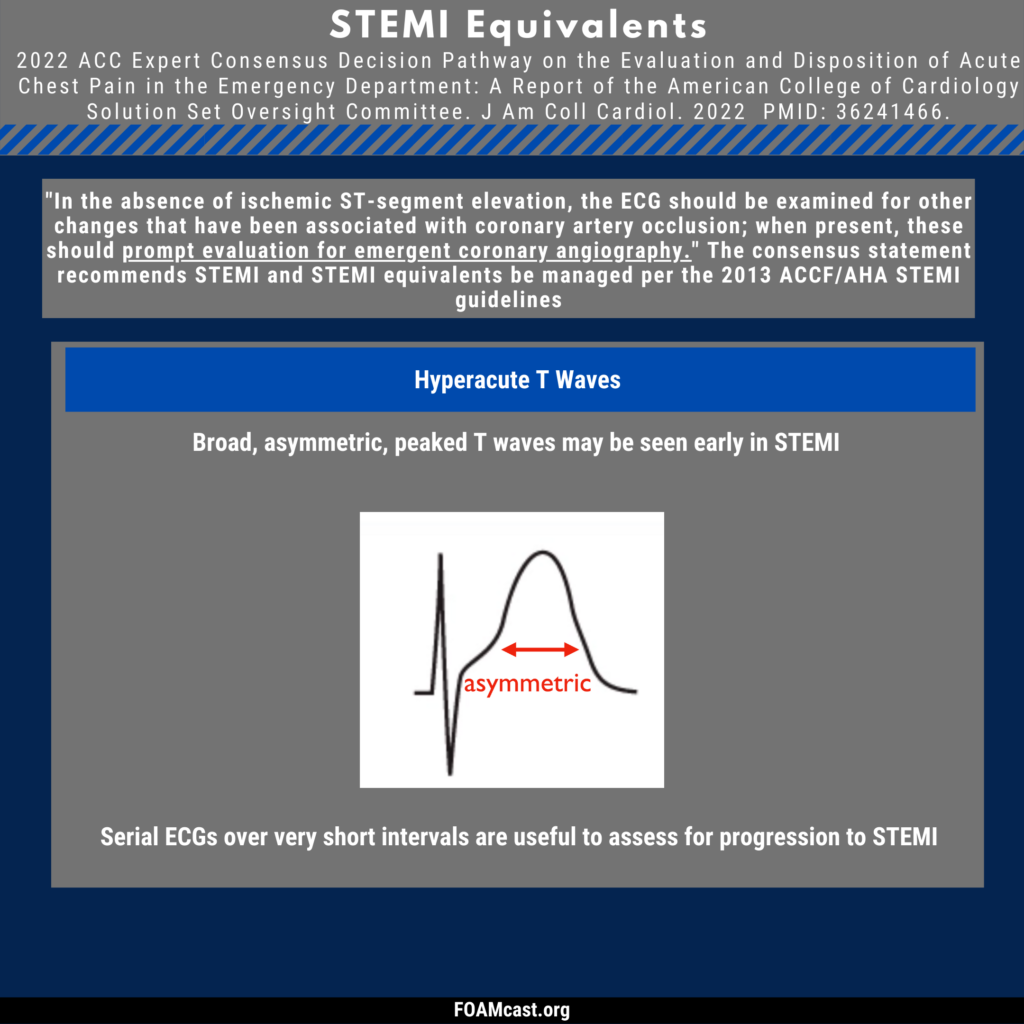
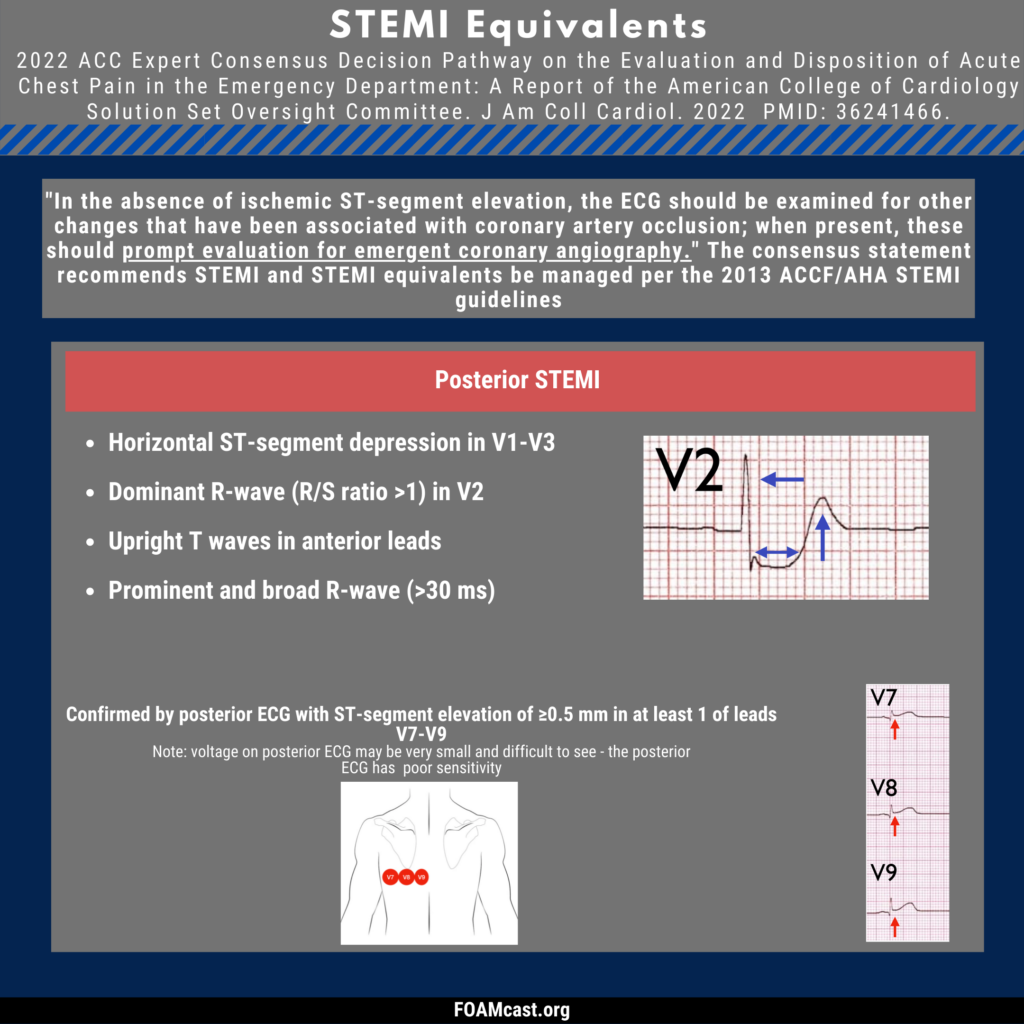
It has become increasingly publicized, primarily due to Stephen Smith and Pendell Meyers, that the STEMI vs NSTEMI dichotomy neglects many patients who may benefit from reperfusion due to Occlusion Myocardial Infarctions. This update incorporates some other signs as “STEMI Equivalents” and recommends these patients be treated just as those with STEMI.
Cummins RO, Hazinski MF. Cardiopulmonary resuscitation techniques and instruction: When does evidence justify revision? Ann Emerg Med. 1999;34(6):780–784.
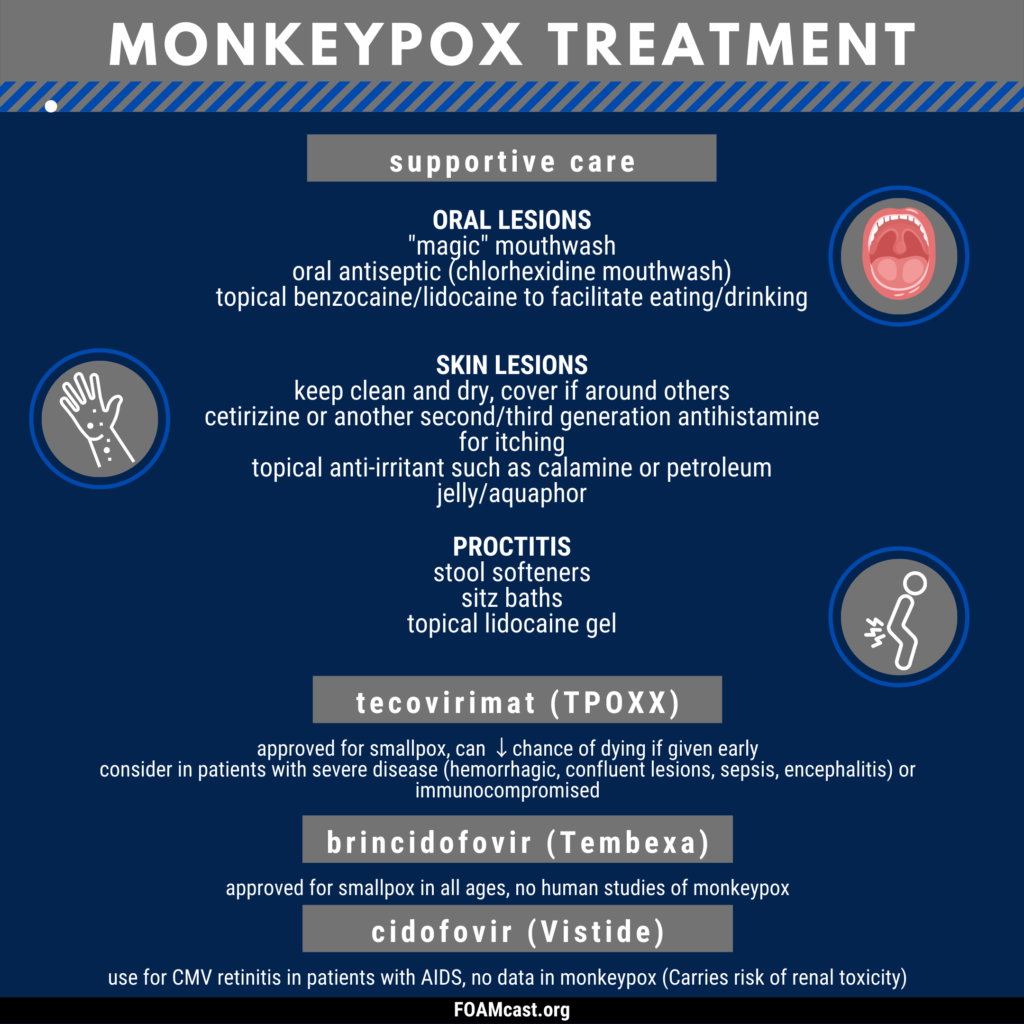
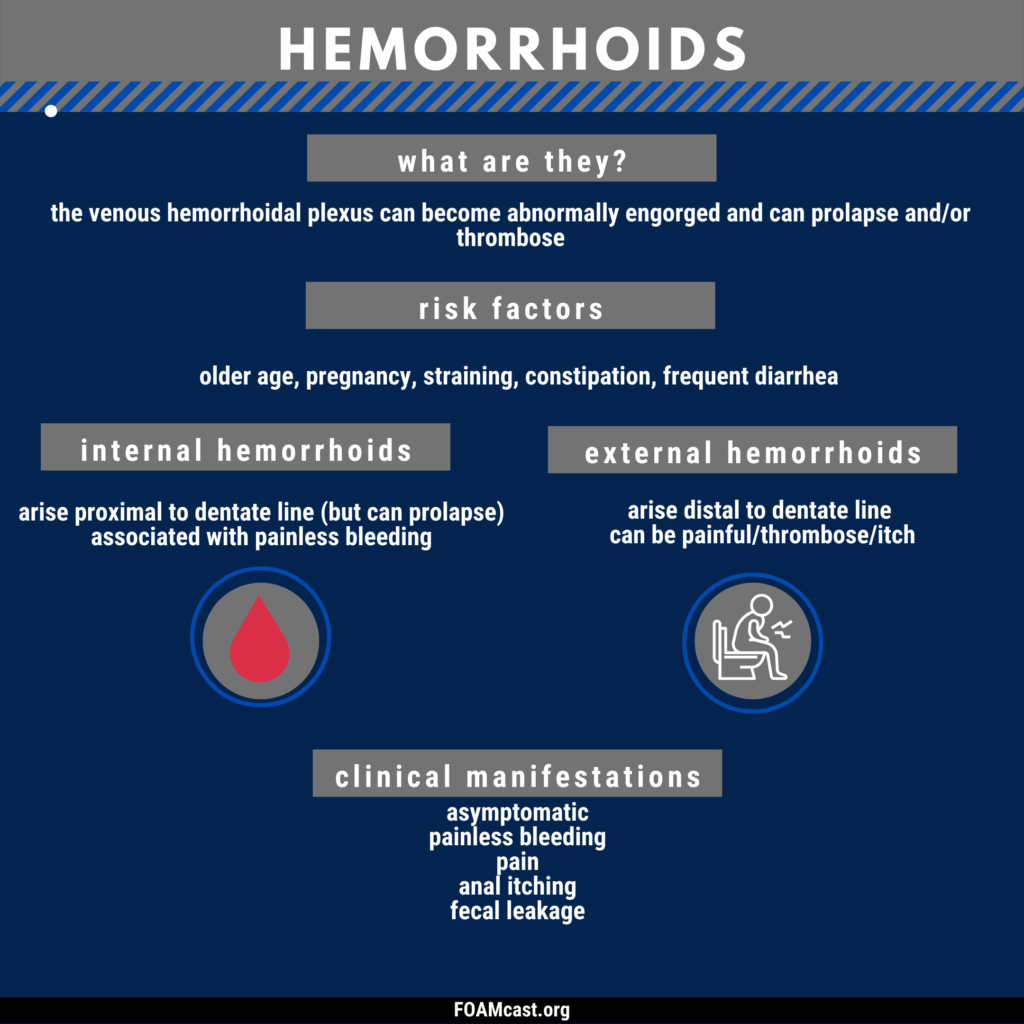
There are practice-changing updates in the guidelines from the World Society of Emergency Surgery (WSES) and American Association for the Surgery of Trauma (AAST), found here. In this podcast, we review hemorrhoids and management.
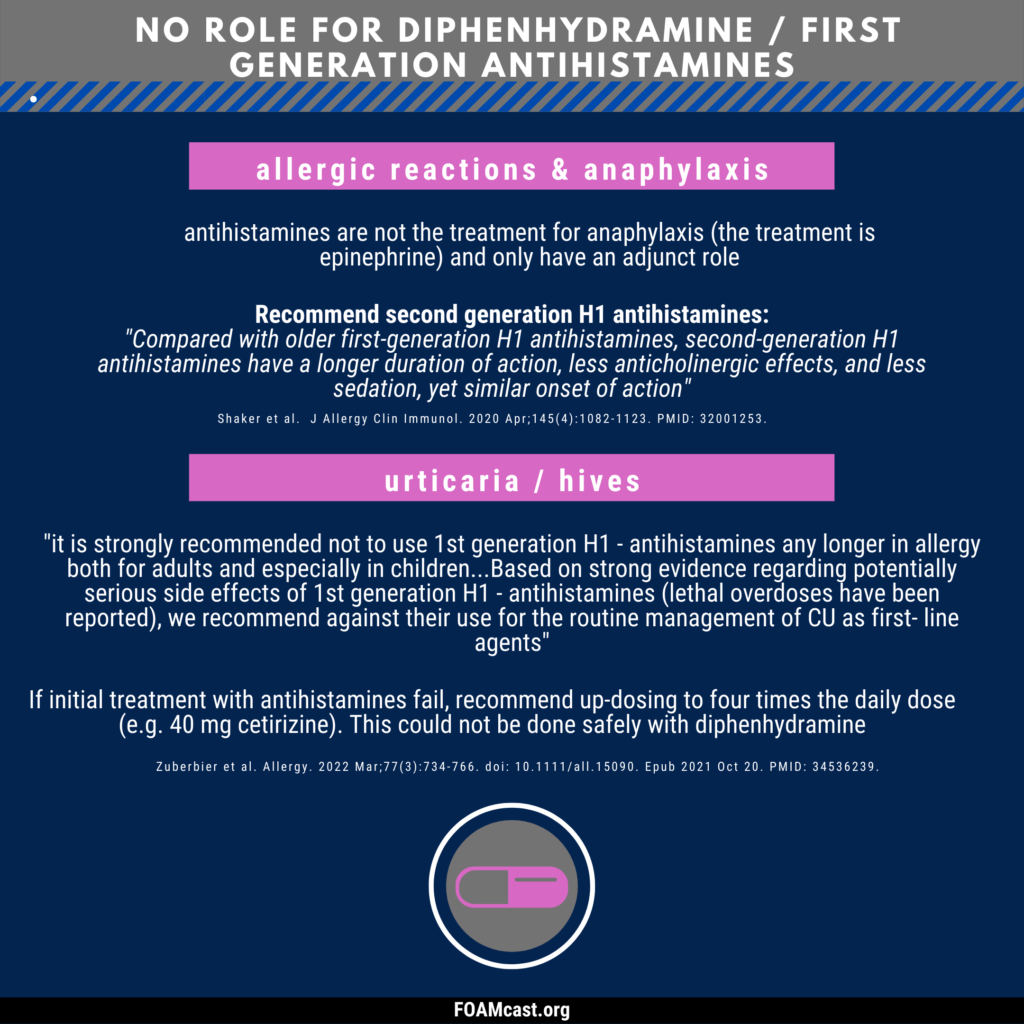
Diphenhydramine and other first-generation antihistamines are ubiquitous in medicine cabinets across the globe. Clinicians commonly recommend or administer diphenhydramine (Benadryl) for a variety of diseases – anaphylaxis, allergic reactions, urticaria, benign headaches/migraines, and as a sleep aid. However, professional societies have recommended against many of these indications for decades and, in other cases, there are safer alternatives. For more reading and references, see this article in ACEPnow.
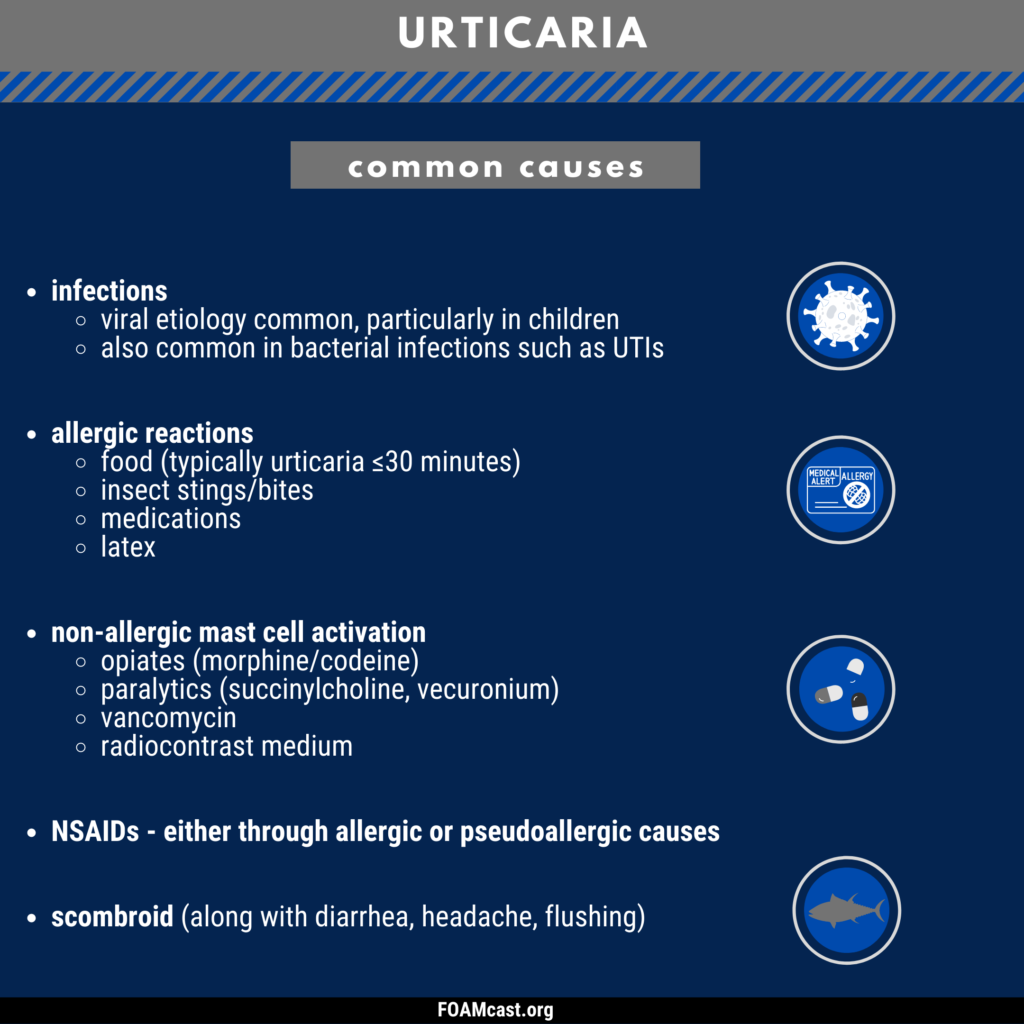
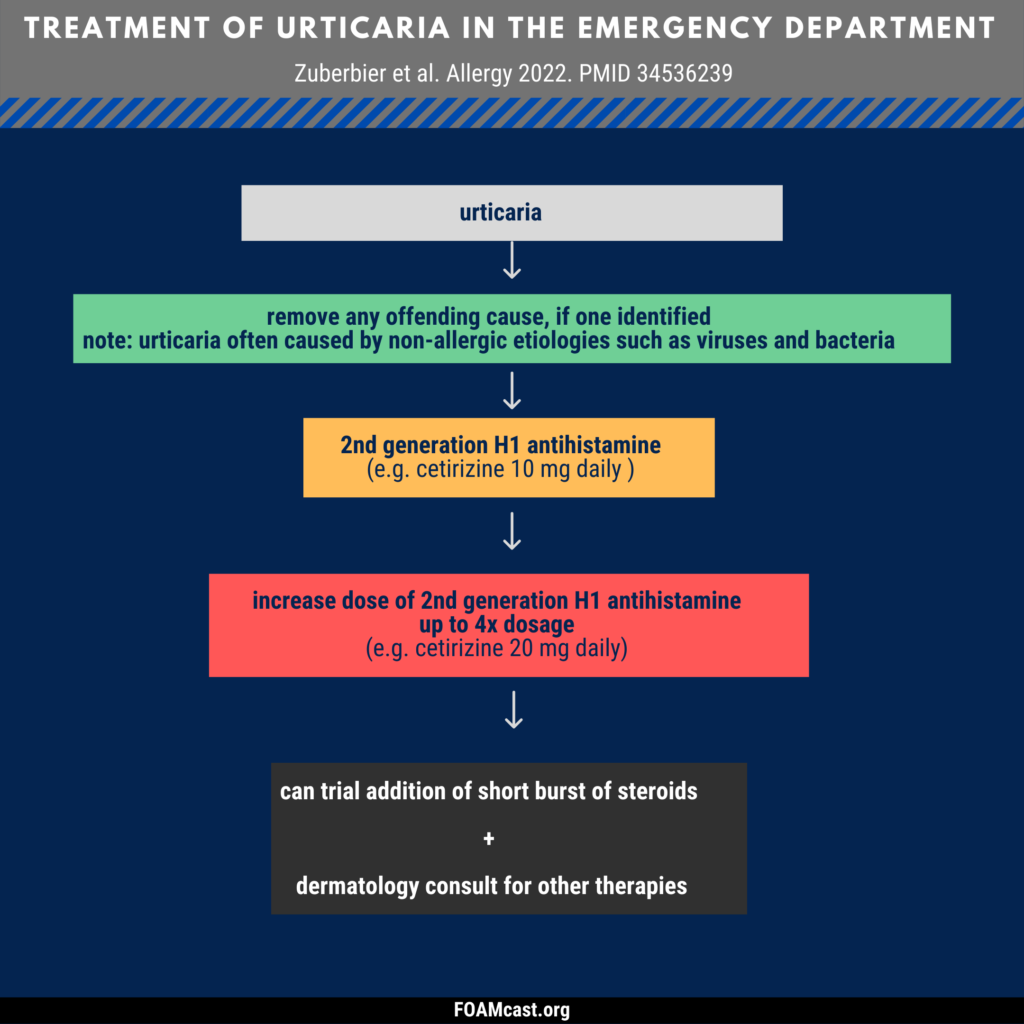
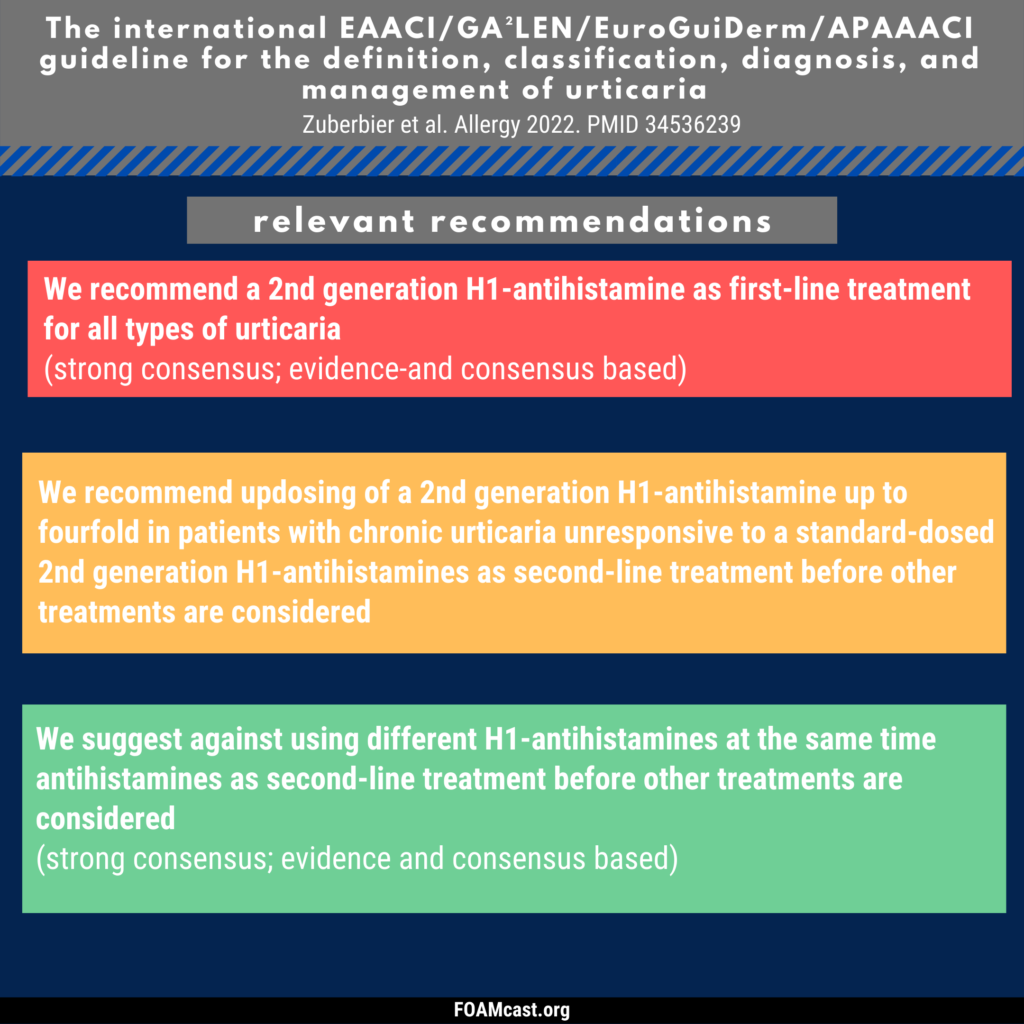
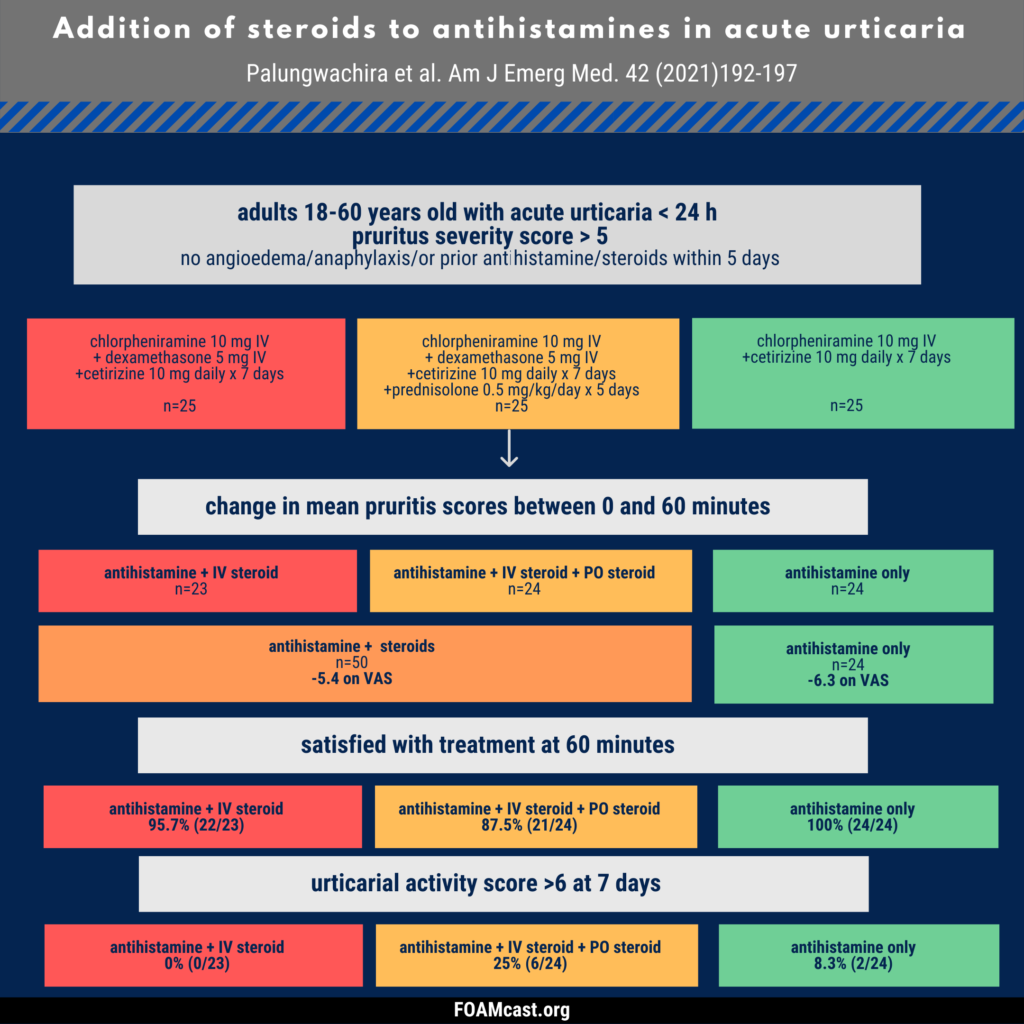
In this podcast, we review acute urticaria (<6 weeks in duration). We review the recent international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria (Zuberbier et al) In addition, we review some of the controversy regarding the administration of steroids for acute urticaria.
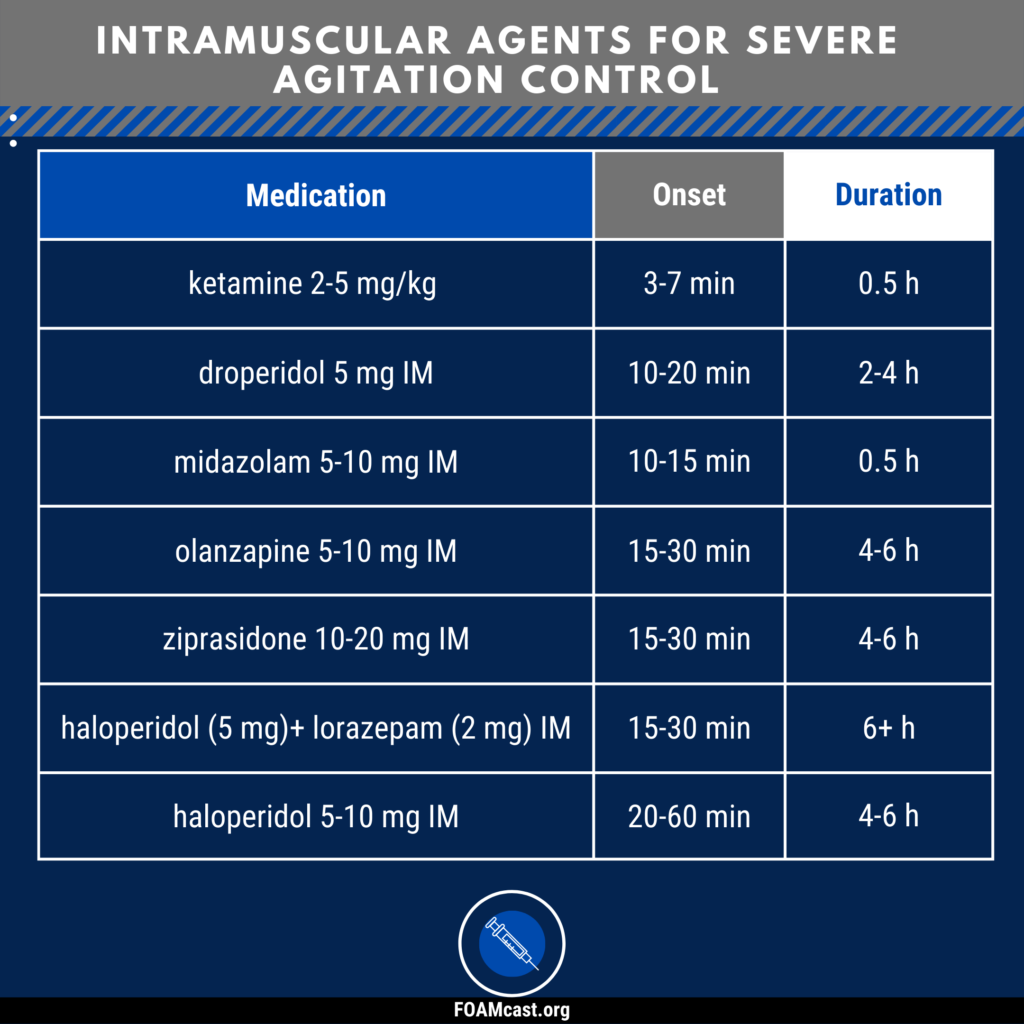
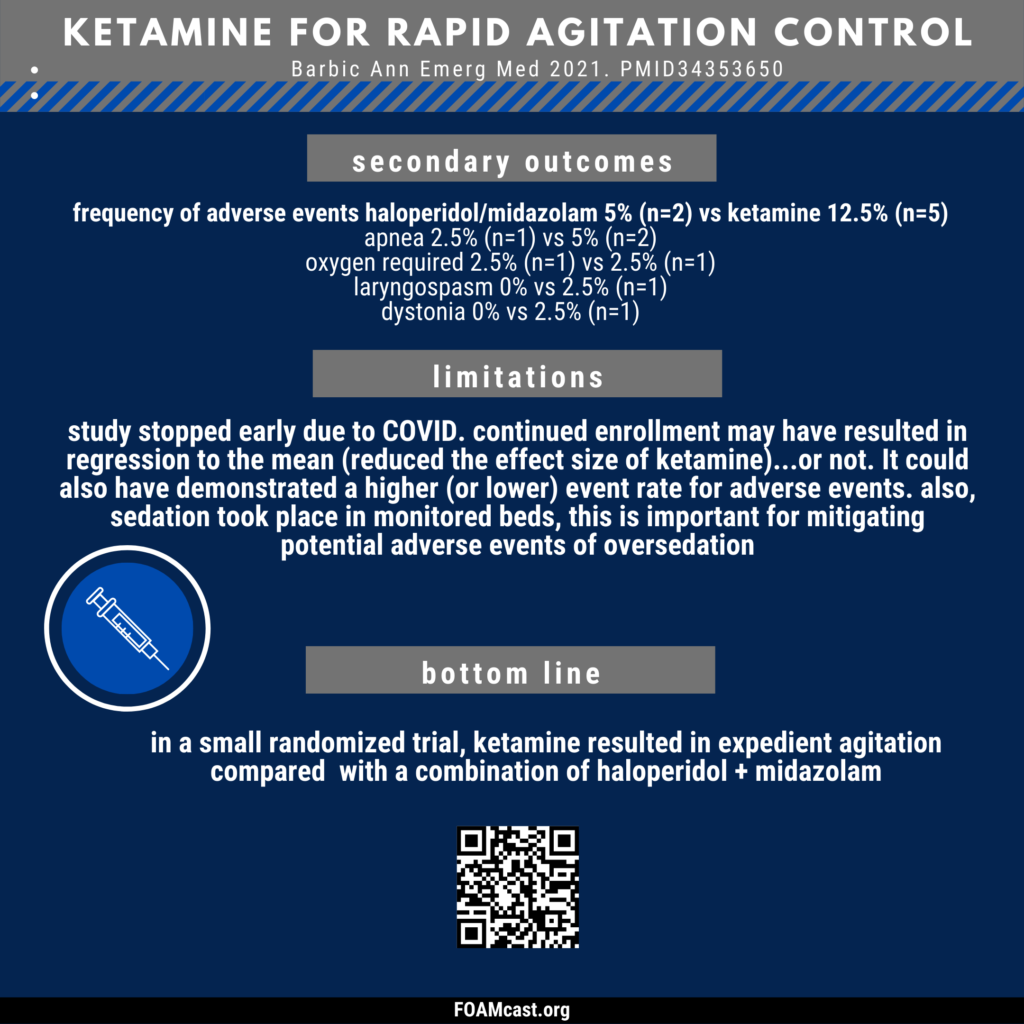
Intramuscular chemical sedation is commonly used in the emergency department (ED) for severe agitation and physical assault when other attempts at de-escalation and agitation control (verbal de-escalation, space, etc) are unsuccessful. The “cocktails” people use are often institution-based. In this podcast, we review commonly used intramuscular agents along with recent papers including ketamine, droperidol, and choice of benzodiazepines.
Droperidol has been cited as working very quickly, however, several studies show that the onset is in the ballpark of 15-20 minutes (even at 10 mg IM).
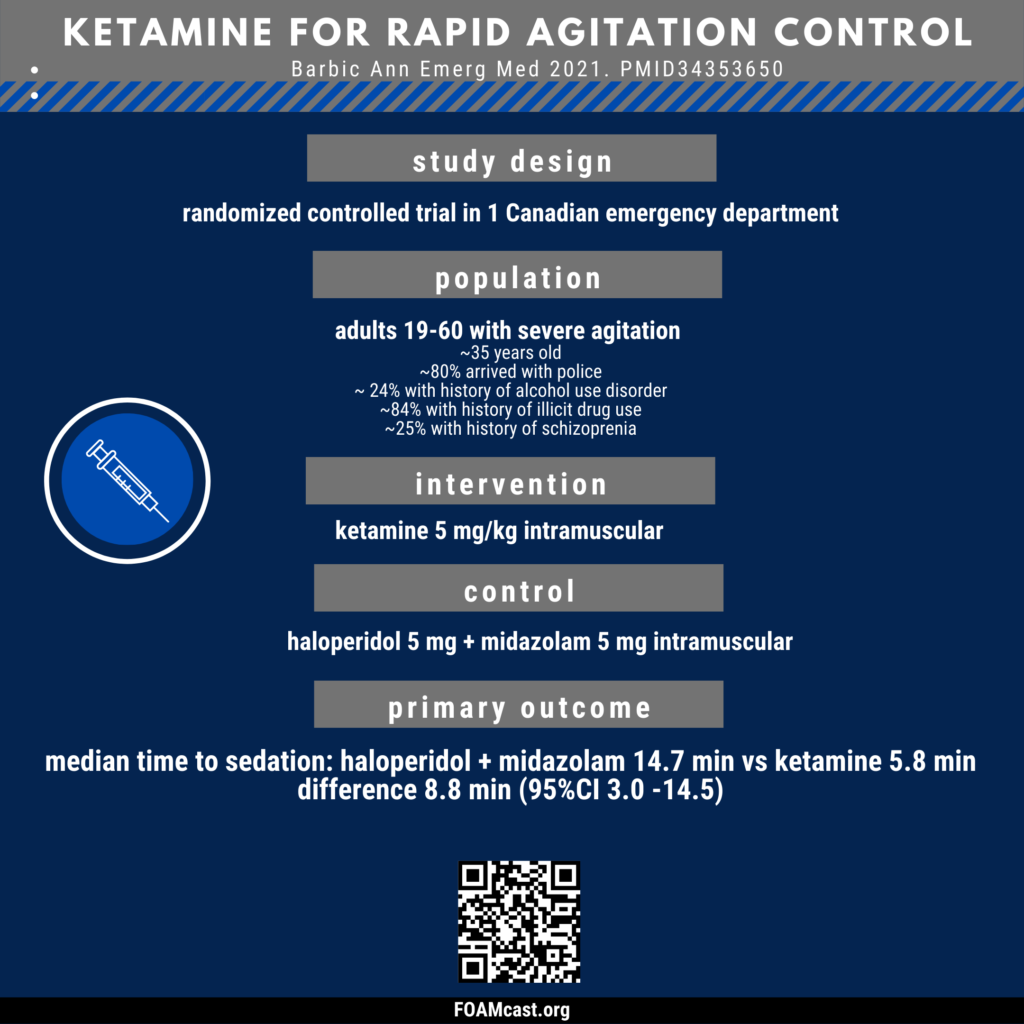
A recent randomized controlled trial of ketamine versus haloperidol + midazolam by Barbic et al demonstrates impressive time to agitation control for ketamine.
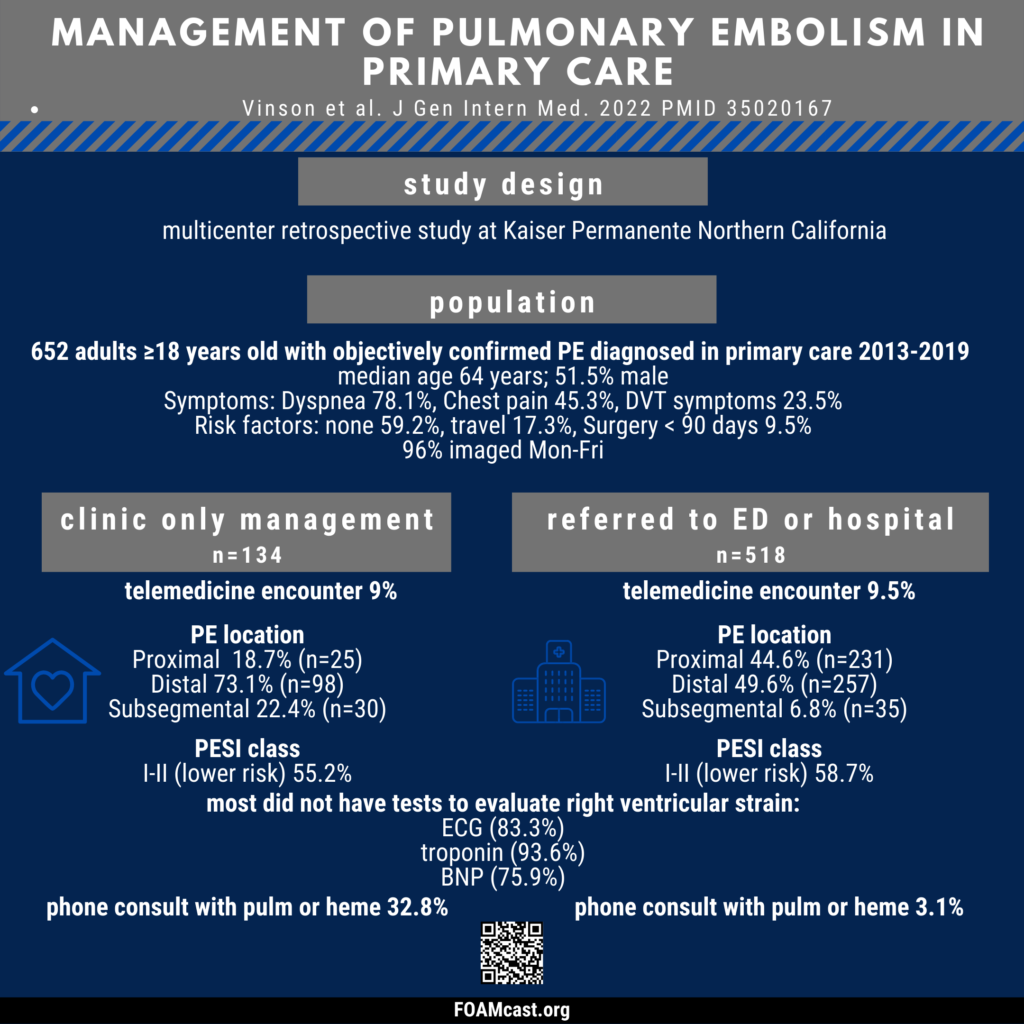
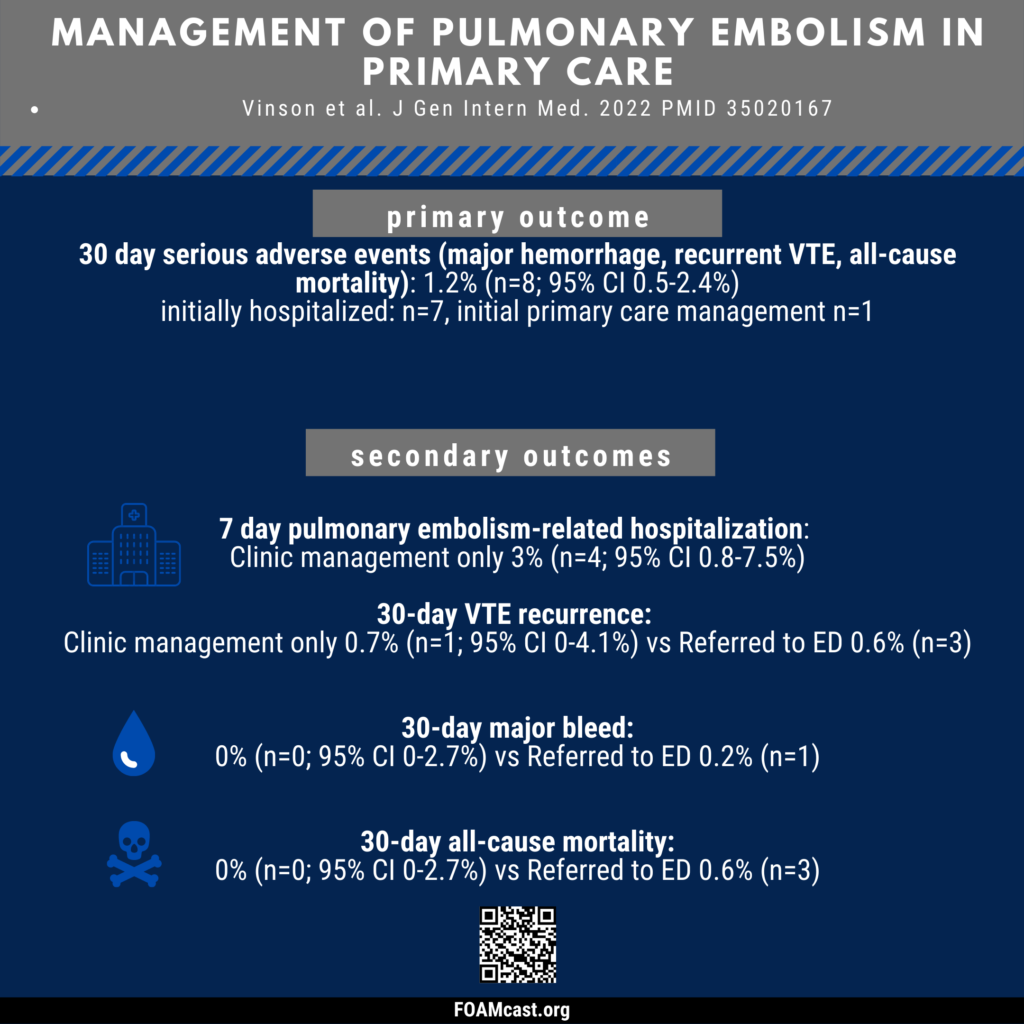
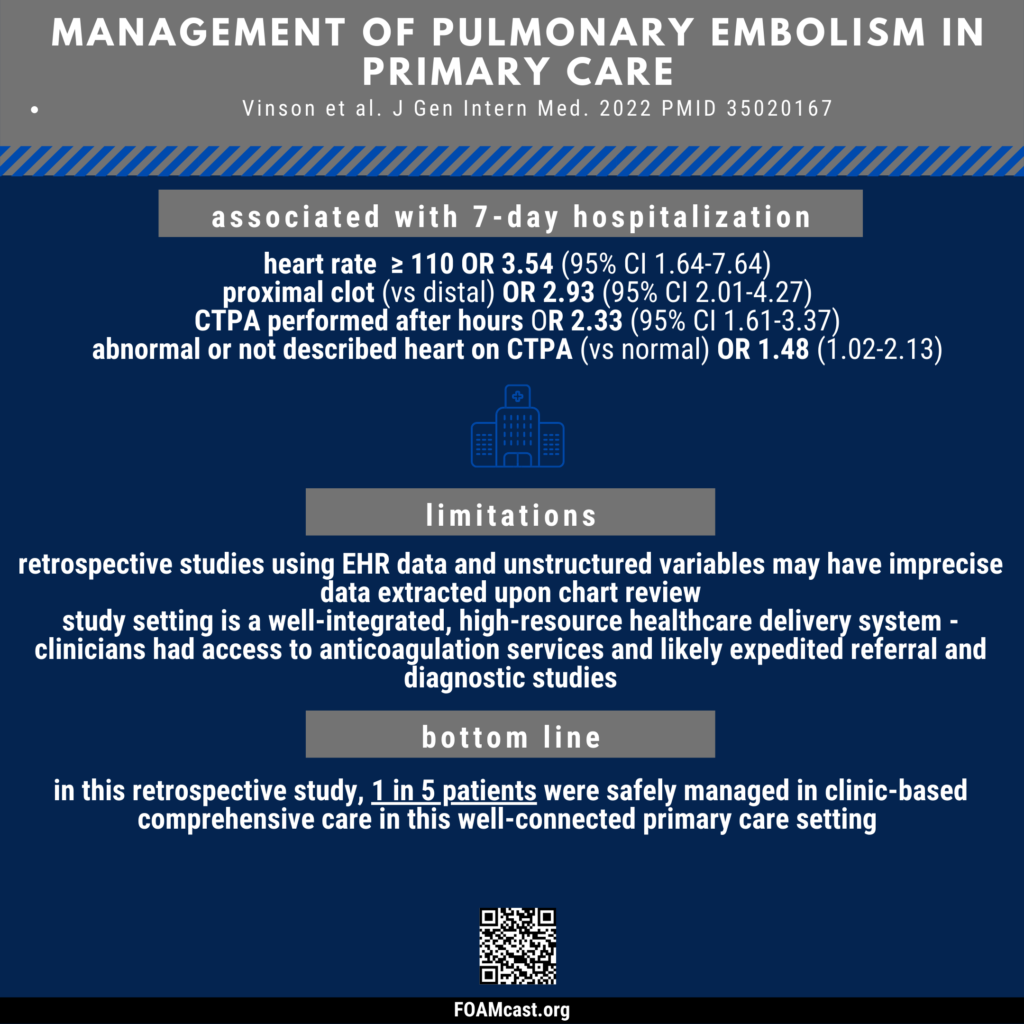
Guidelines have recommended outpatient management for patients with low-risk pulmonary embolism (PE) for many years. Despite this, few patients in the US diagnosed with acute PE are discharged from the Emergency Department (Westafer et al). Little is known about the course of patients managed exclusively or primarily in the outpatient setting. In this study, Vinson and colleagues describe the nature and course of patients diagnosed with pulmonary embolism in the primary care setting.
Vinson DR, Hofmann ER, Johnson EJ, Rangarajan S, Huang J, Isaacs DJ, Shan J, Wallace KL, Rauchwerger AS, Reed ME, Mark DG; PEPC Investigators of the KP CREST Network. Management and Outcomes of Adults Diagnosed with Acute Pulmonary Embolism in Primary Care: Community-Based Retrospective Cohort Study. J Gen Intern Med. 2022 Jan 12. doi: 10.1007/s11606-021-07289-0. Epub ahead of print. PMID: 35020167.
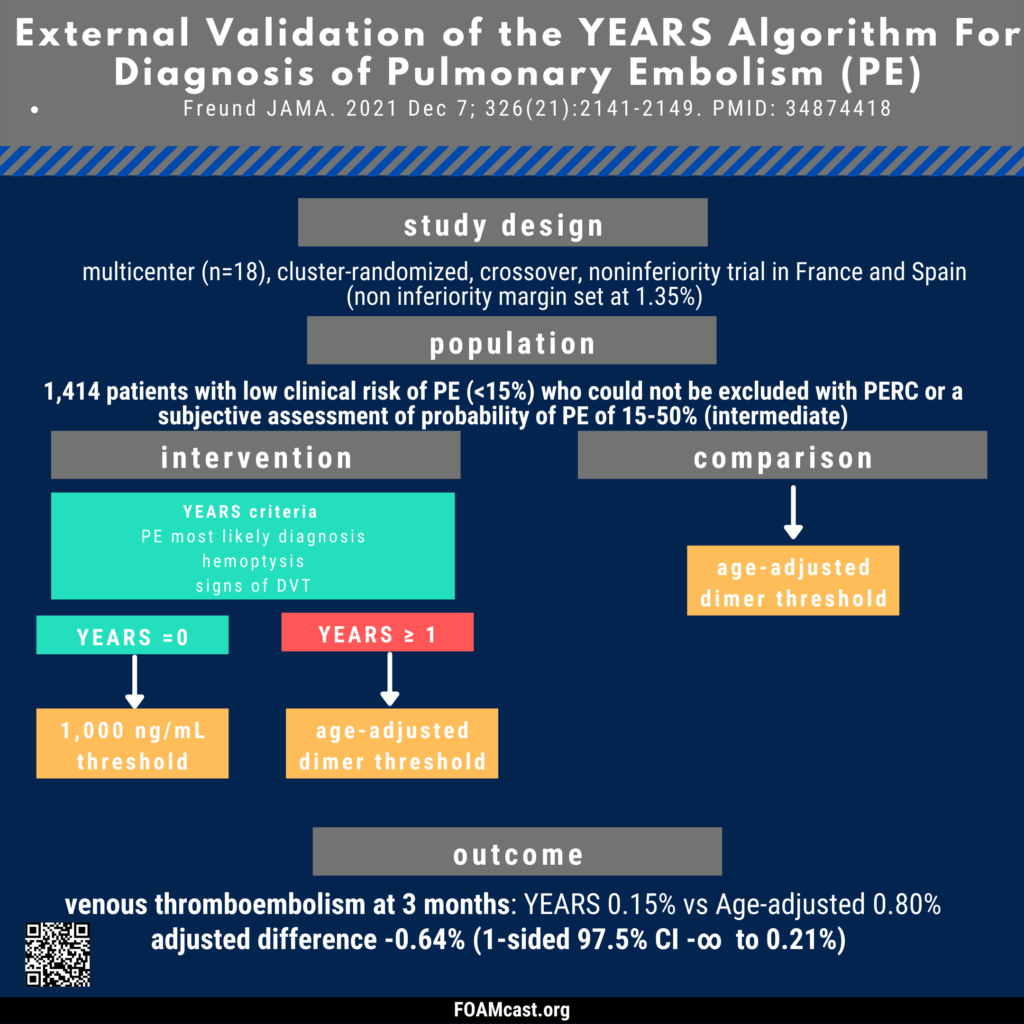
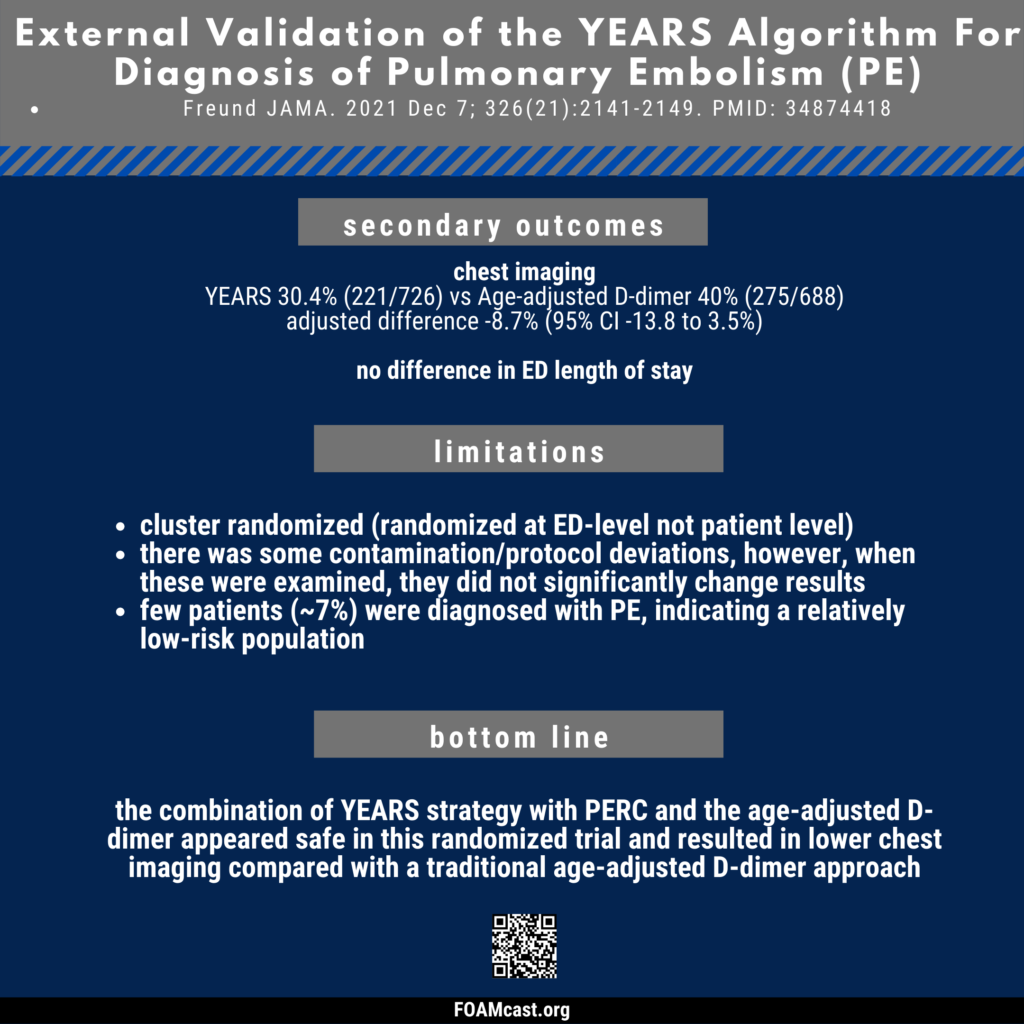
The diagnostic algorithm for pulmonary embolism (PE) has evolved over the past few years to include probability or risk-adjusted D-dimer. The YEARS algorithm includes an elevated D-dimer threshold for some risk groups and has been found to be safe and reduce imaging in several studies, including in pregnant patients. Now, this multicenter trial by Freund et al evaluates the use of YEARS and age-adjusted D-dimer compared with an age-adjusted approach alone.
Freund Y, Chauvin A, Jimenez S, Philippon AL, Curac S, Fémy F, Gorlicki J, Chouihed T, Goulet H, Montassier E, Dumont M, Lozano Polo L, Le Borgne P, Khellaf M, Bouzid D, Raynal PA, Abdessaied N, Laribi S, Guenezan J, Ganansia O, Bloom B, Miró O, Cachanado M, Simon T. Effect of a Diagnostic Strategy Using an Elevated and Age-Adjusted D-Dimer Threshold on Thromboembolic Events in Emergency Department Patients With Suspected Pulmonary Embolism: A Randomized Clinical Trial. JAMA. 2021 Dec 7;326(21):2141-2149. doi: 10.1001/jama.2021.20750. PMID: 34874418; PMCID: PMC8652602.