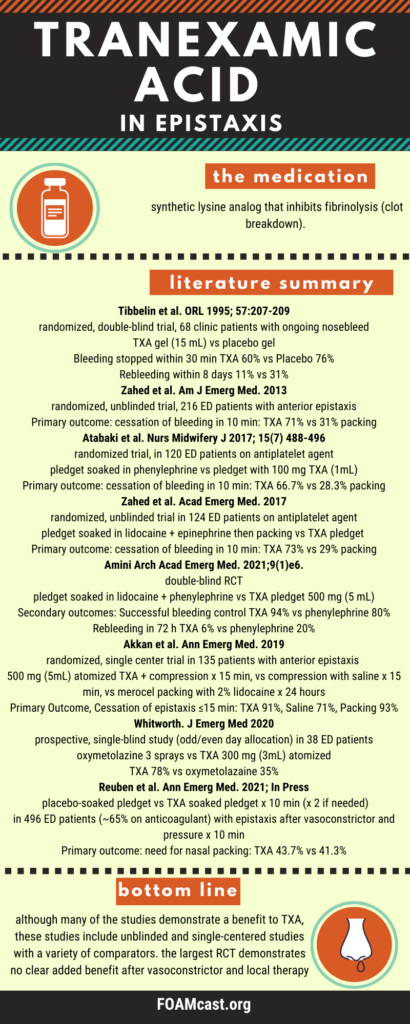
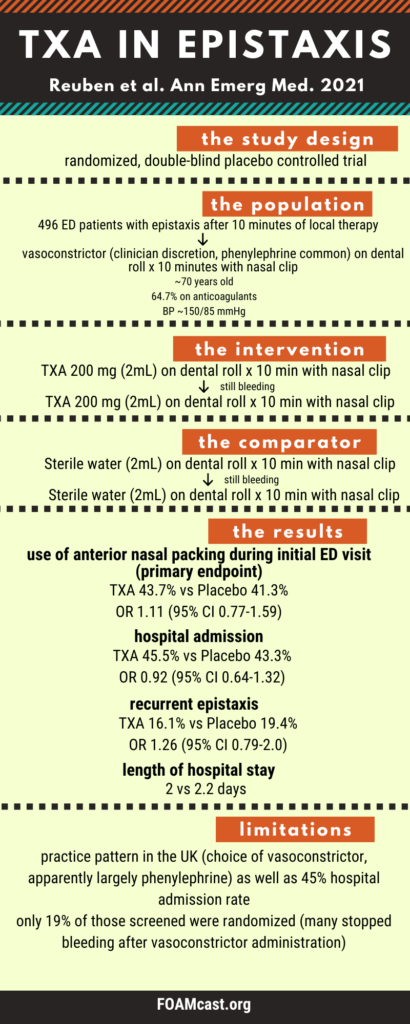
In this episode we cover the literature on tranexamic acid (TXA) in epistaxis, including a new trial in Annals of Emergency Medicine by Reuben et al, the NoPac trial.
Other references include:
Tibbelin et al. Effect of local tranexamic acid gel in the treatment of epistaxis. ORL J Otorhinolaryngol Relat Spec. 1995 Jul-Aug;57(4):207-9. PMID: 7478455.
Zahed et al.A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med. 2013 Sep;31(9):1389-92. doi: 10.1016/j.ajem.2013.06.043. Epub 2013 Jul 30. PMID: 23911102.
Atabaki et al. A Comparative Study on the Effect of Topical Phenylephrine with Topical Tranexamic Acid in Management of Epistaxis. Nurs Midwifery J. 2017; 15 (7) :488-496
Zahed R, et al. Topical Tranexamic Acid Compared With Anterior Nasal Packing for Treatment of Epistaxis in Patients Taking Antiplatelet Drugs: Randomized Controlled Trial. Acad Emerg Med. 2018 Mar;25(3):261-266. doi: 10.1111/acem.13345. Epub 2017 Dec 9. PMID: 29125679.
Akkan S et al. Evaluating Effectiveness of Nasal Compression With Tranexamic Acid Compared With Simple Nasal Compression and Merocel Packing: A Randomized Controlled Trial. Ann Emerg Med. 2019 Jul;74(1):72-78. doi: 10.1016/j.annemergmed.2019.03.030. Epub 2019 May 9. PMID: 31080025.
Amini et al. Topical Tranexamic Acid versus Phenylephrine-lidocaine for the Treatment of Anterior Epistaxis in Patients Taking Aspirin or Clopidogrel; a Randomized Clinical Trial. Arch Acad Emerg Med. 2020 Nov 19;9(1):e6. PMID: 33313573; PMCID: PMC7720853.
Whitworth et al. Comparative Effectiveness of Topically Administered Tranexamic Acid Versus Topical Oxymetazoline Spray for Achieving Hemostasis in Epistaxis. J Emerg Med. 2020 Feb;58(2):211-216.
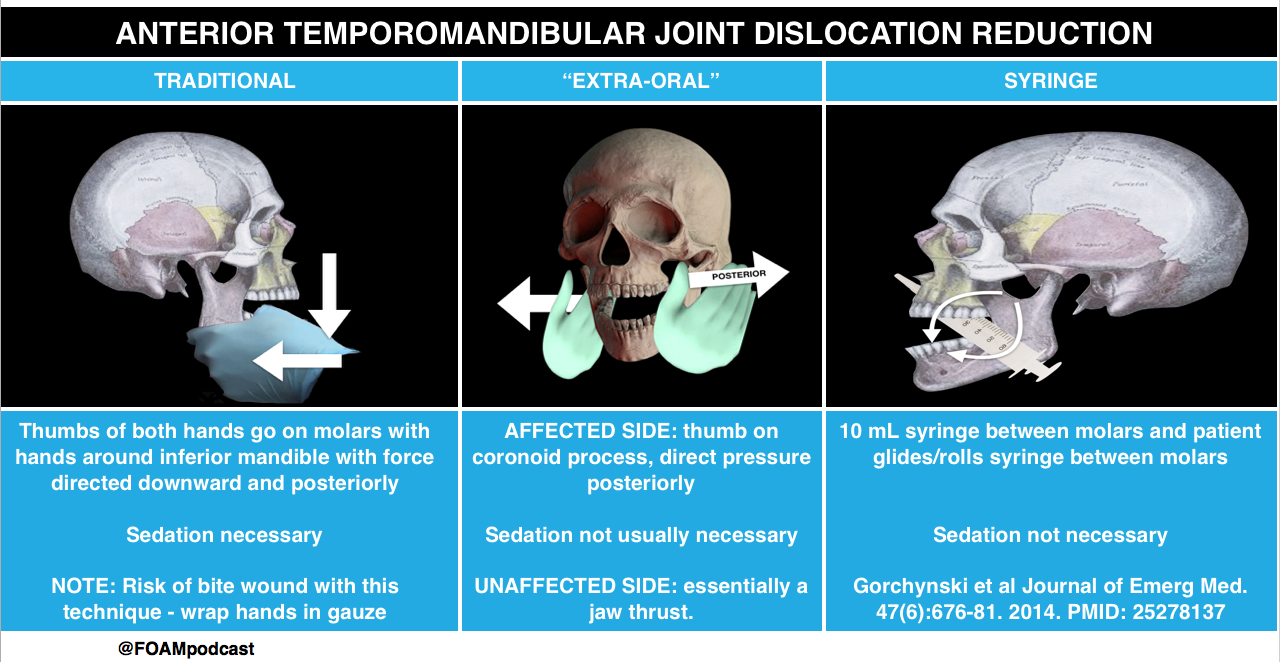
Traditional Approach to TMJ dislocation and Syringe Technique from Core EM
Core Content
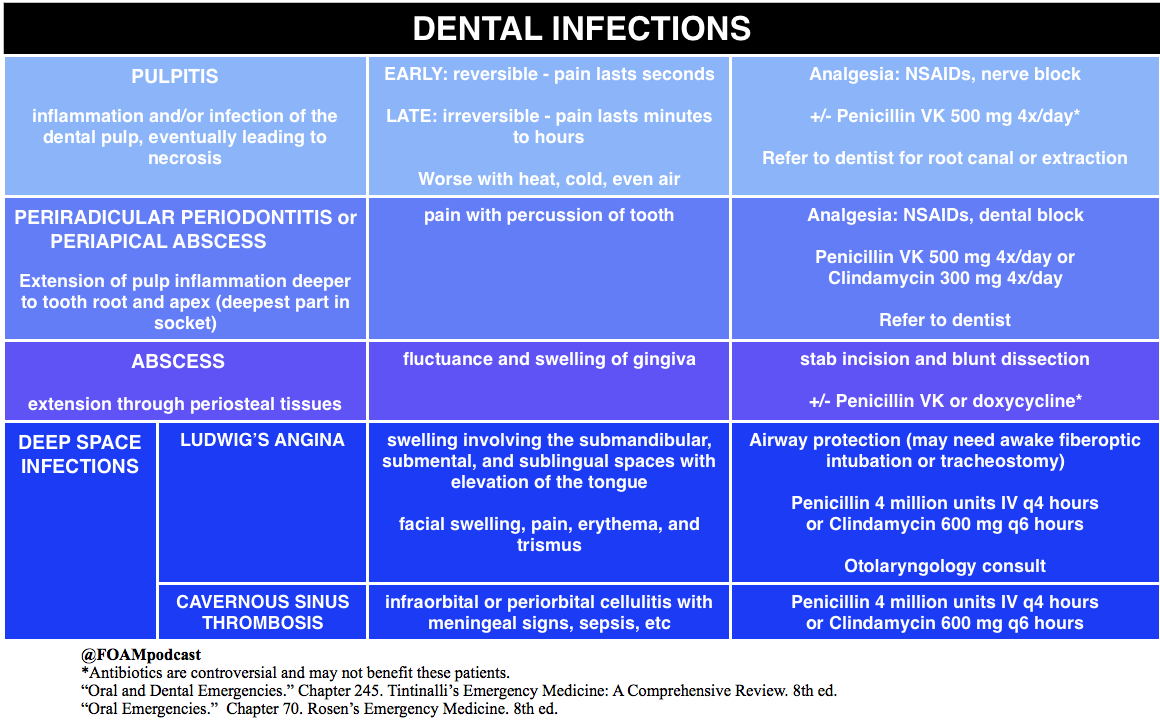
We delve into core content on dental injuries using Rosen’s Emergency Medicine (8th edition) Chapter 70 “Oral Emergencies” and Tintinalli’s Emergency Medicine (8th edition) Chapter 245 “Oral and Dental Emergencies” as a guide.
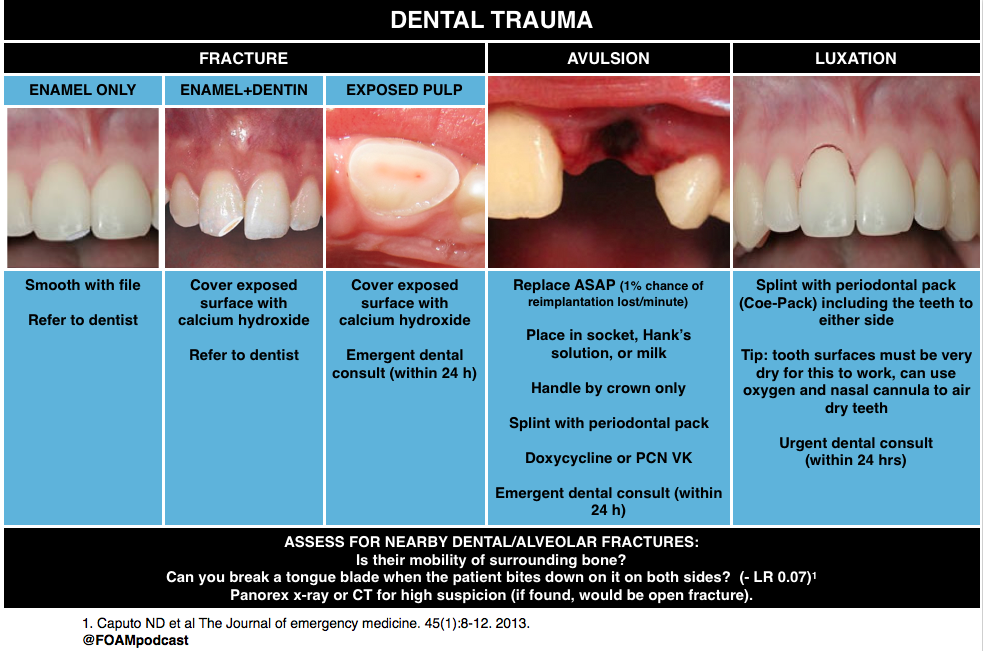
A 19-year-old man presents to the Emergency Department with an avulsed tooth. He struck his mouth on the back of another player’s head while playing basketball. He arrives thirty minutes after the injury with his right maxillary central incisor in a bag of cold milk. Which of the following is the most appropriate management?
C. Reimplant the avulsed tooth (B) is the most appropriate next step. Avulsed permanent teeth should be reimplanted as soon as possible, ideally within 30 minutes of the injury. For every minute that the tooth is out of its socket, there is a 1% chance of reimplantation failure. If the tooth is not able to be reimplanted immediately, it should be stored in an appropriate medium. Cold milk is preferable to sterile water or saliva as it has magnesium and calcium. Hank’s solution, a neutral cell culture medium, is ideal. Once the tooth is reimplanted, the tooth should be stabilized until dental follow up is arranged. Avulsed primary teeth should not be reimplanted.
[/toggle]
[/accordion]
A 25 year-old man presents after falling face forward off his bike. He sustained an abrasion inside his upper lip and complains of a broken front tooth. He brought the fractured fragment with him. On examination, the bony structures of the jaw are non-tender. There is no malocclusion. Tooth #8 has a fracture and in the center of the exposed area is a small pink dot. What is the most appropriate plan for this patient?
A. Dental follow-up within the next 24 hours
B. Irrigation of the tooth
C. Placement of the tooth fragment in Hank’s solution
A. This patient has a dental fracture with exposed pulp. This is a dental emergency requiring dental follow-up within the next 24 hours. The most superficial dental fractures involve only the enamel on the surface and treatment is mostly cosmetic and aimed at dulling any sharp edges. Fractures that expose dentin will have an ivory-yellow appearance. In younger patients, there is less dentin relative to the pulp and treatment is aimed at protecting any pulp contamination with placement of a calcium-hydroxide dressing. Younger patients need more urgent follow-up with a dentist. The most significant dental fractures involve the pulp as in this clinical scenario. The tooth should be gently wiped clean with gauze and inspected for a drop of blood or pink blush which represents pulp exposures. The area is usually exquisitely painful. Timely follow-up (within 24 hours) is required for evaluation and possible root canal and extraction of the pulp. If dental follow-up will be delayed, the tooth should be covered with moist cotton and sealed with dry foil or a temporary commercial sealant. In order to clean the tooth, a clean gauze should be used to wipe off the surface, not irrigation of the tooth (B) as the patient will be extremely sensitive to that and all efforts should be maintained to avoid pulp contamination. Hank’s solution (C) is a physiologic solution in which an avulsed tooth may be placed while waiting for reimplantation into the socket. There is no role in a partial tooth fracture. Viscous lidocaine (D) is not an appropriate analgesic for a dental fracture. Oral analgesics or dental block should be provided for pain control.
[/toggle]
[/accordion]
References
Gorchynski J, Karabidian E, Sanchez M. The “syringe” technique: a hands-free approach for the reduction of acute nontraumatic temporomandibular dislocations in the emergency department. The Journal of emergency medicine. 47(6):676-81. 2014. [pubmed]
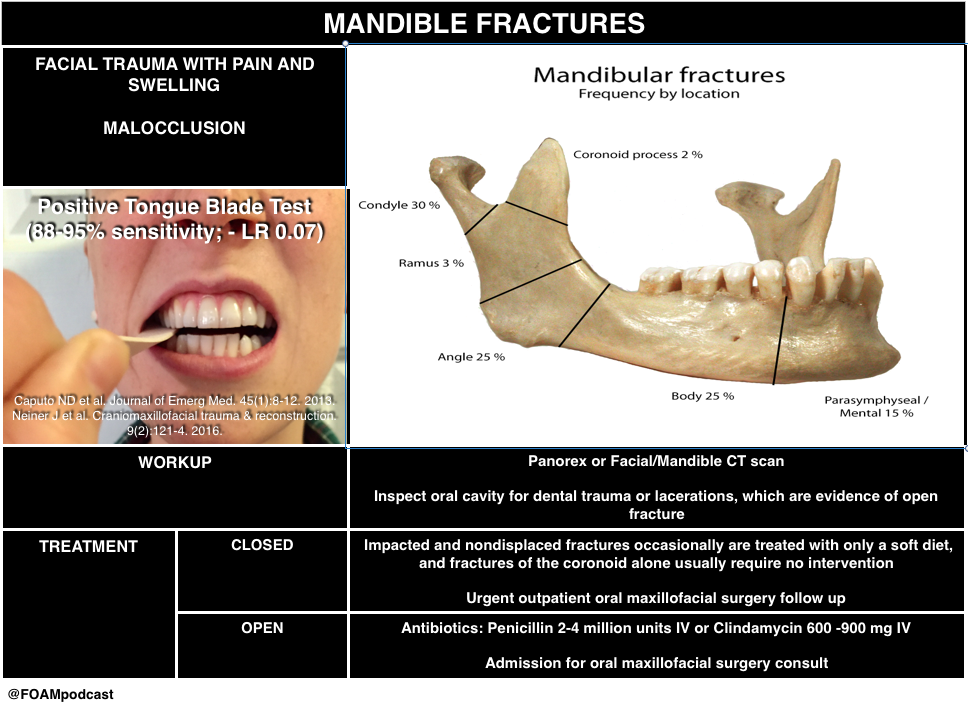
Caputo ND, Raja A, Shields C, Menke N. Re-evaluating the diagnostic accuracy of the tongue blade test: still useful as a screening tool for mandibular fractures? The Journal of emergency medicine. 45(1):8-12. 2013. [pubmed]