(ITUNES OR LISTEN HERE)
The Free Open Access Medical Education (FOAM)
We review the Tox Talk podcast, Episode 23 – Mushrooms. Our favorite pearls:
Clitocybe, Inocybe – contain muscarine which stimulates muscarinic receptors (acetylcholine/parasympathetic), causing a cholinergic toxidrome. Think SLUDGE (salivation, lacrimation, urination, defecation, gastric emptying/emesis) and the Killer B’s (bradycardia, bronchorrhea, bronchospasm) or DUMBELLS (diarrhea/diaphoresis, urination, miosis, bradycardia, emesis, lacrimation, lethargy, salivation). Basically, cholinergic toxidrome: SMALL, WET, SLOW.
- Memory aid: these mushrooms end in -yBE, akin to the “killer B’s” that make cholinergic toxicity deadly.
Gyromitra – (false morel) contains gyromitrin which can cause seizures, in addition to gastrointestinal upset and liver failure. Treatment: pyridoxine (B6).
- Memory aid: gyromitra named because they look like the gyri of the brain and, conveniently, make the brain seize through depletion of GABA.
Amanita phalloides – contains amatoxins which cause delayed gastrointestinal symptoms and liver failure., echoing acetaminophen toxicity.
- Caution: this is different than the amanita muscaria ‘mushroom, which is tricky because that amanita muscaria has neither muscarinic properties nor the toxicity of amanita phalloides.
Bonus pearl: Coprinus species can cause a disulfiram like reaction.
FOAM article on mushrooms by Jo et al
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter ; Rosen’s 8(e) Chapter – but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Hypothermia starts at 35°C and then is categorized based on severity.

Pearls:
- Ethanol + hypothermia = bad news. Ethanol is the most common cause of excessive heat loss in urban areas as people tend to not take warming measures, may be homeless or without heat, and have impaired thermoregulation. Hypothermia also slows alcohol metabolism, making people drunker for longer.
- Elderly patients are more susceptible to hypothermia, particularly as they may not sense the cooler temperatures. Some may also have impaired thermoregulation.
- Have a low threshold
Diagnostics:
- Get a temperature, on all patients. This applies to patient’s “found down” as well as the chronic alcoholic who just seems really drunk.
- If patients aren’t rewarming 1°C/hr and they’re above 32°C, consider: sepsis, cortisol deficiency, myxedema, ethanol.
- The J wave or “Osborn” wave is found in many cases of hypothermia, often quoted at ~80%. However, it is not pathognomonic for hypothermia.

Treatment: Warm the patient. Don’t call the patient dead until they’re warm and dead, which means their temp is above 30-32°C.
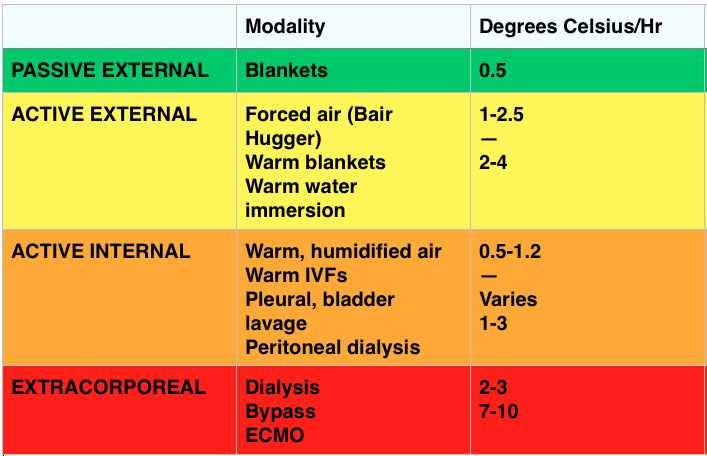
Passive Rewarming – effective when the patient can still shiver (33-35°C).
- Generates ~1.5°C of heat/hr
Active Rewarming – direct transfer of heat to the patient.
- Indications: Cardiovascular instability, temp ≤30-32° C, inadequate rate of rewarming or failure to rewarm, endocrine problem, trauma, tox, secondary hypothermia impairing thermoregulation
- Can be external or internal (which can be minimally invasive like IV fluids or quite invasive with things like bypass or pleural lavage).
Outcomes –
- Unlikely survival with a potassium > 12 mmol/L and recommendations are to terminate resuscitation for potassium >12 mmol/L and consider cessation for potassium between 10-12 mmol/L
FOAM Resources:
EBM Gone Wild on Prognostication
ScanCrit on ECMO in Accidental Hypothermia
EMCrit on Severe Accidental Hypothermia
Generously Donated Rosh Review Questions (Scroll for Answers)
Question 1. A 40-year-old man with a history of substance abuse is brought in by EMS after being found unconscious outside of a nightclub in the middle of winter. It is unclear how long he was outside. He is unresponsive with a GCS of 3.[polldaddy poll=8469565]
Question 2. What is the most common cause of death in hypothermic patients after successful resuscitation?
Question 3.

[polldaddy poll=8473489]
Question 4. What abnormal rhythm is common with temperatures below 32°C?
References:
Danzl DF, Zafren K. Accidental Hypothermia, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 7. St. Louis, Mosby, Inc., 2013, (Ch) 140: pp 1883-1885.
Brown D JA, Brugger H, et al. Accidental Hypothermia. N Engl J Med 2012;367:1930-1938.
Mair P, Kornberger E, et al. Prognostic markers in patients with severe accidental hypothermia and cardiocirculatory arrest. Resuscitation 1994;27:47-54.
Answers:
1. D. When the serum potassium is greater than 12 mmol/L resuscitative efforts should be halted as the patient is unlikely to survive and further efforts constitute futile care. Accidental hypothermia is not an uncommon occurrence particularly in colder climates. It may occur in conjunction with substance abuse when an individual becomes impaired and is subsequently exposed to the outdoors. It can also occur as a result of drowning, avalanche and other trauma. Bio-makers other than potassium have been studied including serum lactate (B), pH (C) and clotting time. None have been proven prognostically reliable and therefore should not be used as a guide to determine if resuscitation should be continued. Hypothermic patients that present in cardiac arrest should be warmed to a minimum of 32°C (A) preferably via ECMO or cardiopulmonary bypass. However, if a hypothermic patient is warmed to 32°C and remains in asystole, recovery is unlikely and resuscitative efforts should be terminated. Other indications to cease resuscitative efforts include: obvious signs of irreversible death (e.g. major trauma), valid DNR order, conditions that are unsafe for the rescuer or provider, and an avalanche burial > 35 minutes in which the airway is packed with snow and the patient is asystolic.
2. Pulmonary edema.
2. C. Hypothermia. The ECG demonstrates the presence of J waves or Osborn waves which are seen in hypothermia. One of the first cardiac effects of hypothermia is bradycardia secondary to decreased firing of the cardiac pacemaker cells in cold temperatures. Osborn waves may appear at any temperature below 32°C. The waves are an upward deflection at the terminal portion of the QRS complex. They may represent abnormal ion flux in cold temperatures along with delayed depolarization and early repolarization of the left ventricular wall. As temperatures continue to drop, the ECG will demonstrate prolonged intervals: PR, followed by QRS and then QTc. Both diabetic ketoacidosis (A) and digoxin toxicity (B) may lead to hyperkalemia. In diabetic ketoacidosis, hyperkalemia develops as a result of the acidic pH in the blood and the transport of hydrogen ions intracellularly in exchange for a potassium ion. Digoxin toxicity poisons the cellular Na+/K+ ATPase resulting in elevated extracellular levels of potassium. The ECG manifestations of hyperkalemia begin with peaked T waves. Multiple other findings eventually develop including a shortened QT interval, ST depression, bundle branch blocks, widened QRS, prolonged PR interval, flattened T wave and ultimately a sine wave. Hyperparathyroidism (D) may lead to hypercalcemia. In hypercalcemia, the ECG shows a shortened QT interval, flattened T waves and QRS widening at very high levels.
4. Atrial fibrillation.