We are at SMACC in Dublin – thanks to the Rosh Review, an excellent board review question bank.
Do We Make Saves?
Dr. Mervyn Singer “Is Survival Predetermined in the Critically Ill?”
- Many critical care studies are negative, but in some cases this may be because critically ill patients don’t have a uniform prognosis.
- Dr. Singer argues that some people may be “destined to die” and some may be “destined to live.” Interventions may be harmful or futile in one group but beneficial in the other. For example, Dr. Singer references the CORTICUS trial of steroids in septic shock [1]. This was a negative trial. Dr. Singer asserts that some evidence (of not great quality), purports that the sickest patients could benefit from steroids, while this same intervention could be deleterious in the healthier ones.
- Problem: many of the studies that go back and re-analyze these groups looking at the sickest or least sick patients? They perform subgroup analyses, a form of data dredging that must be taken with a huge grain of salt.
Favorite Pearls
Dr. Suzanne Mason – “Acute Care of the Elderly”
- Hospital admission may not benefit geriatric patients – interdisciplinary interventions involving nurses, consultants, pharmacists, physical therapy may be best.
- If there is a single, free intervention that providers can do it’s assessing for polypharmacy. Polypharmacy in the elderly is a huge problem. Check the patient’s medication list and beware adding new medications that may not be absolutely necessary.
Dr. Victoria Brazil – “So You Think You’re a Resuscitationist?”
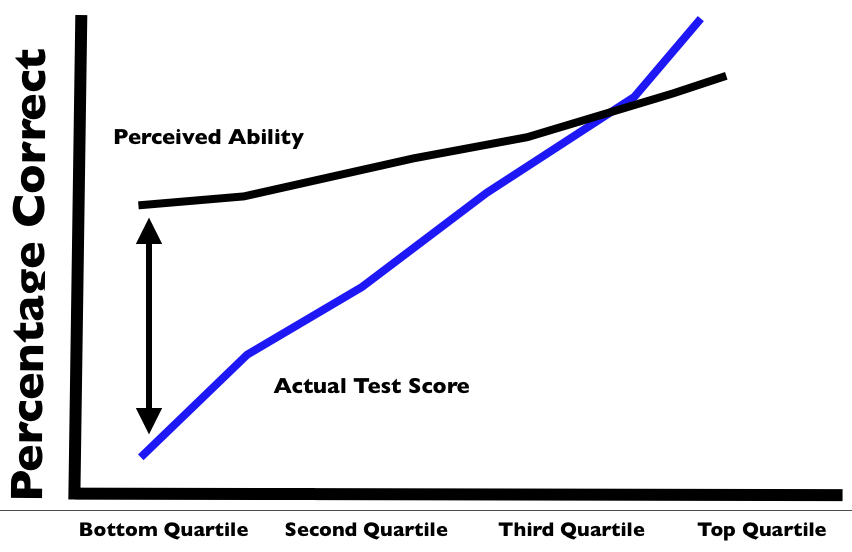
- The Dunning-Kruger effect is real in medicine and this is why we MUST have and provide feedback. A review of the Dunning-Kruger effect can be found here. Essentially, people tend to overestimate what they know (i.e. overly confident in their knowledge). The exception? Masters tend to underestimate their knowledge.
- Our perception of reality is very skewed so, again, feedback is crucial. For example, Cemalovic and colleagues found that intubators underestimated the time they took to intubate: they estimated 23.5 seconds on average vs the 45.5 seconds intubation actually took. Additionally, they thought 13% of their patients desaturated during intubation but 23% actually desaturated [2].
Also, there was an excellent tribute to the late Dr. John Hinds, a reminder that by living profoundly, you can impact people across the world.
References
- Sprung CL, Annane D, Keh D et al. Hydrocortisone Therapy for Patients with Septic Shock. N Engl J Med. 358(2):111-124. 2008. [article]
- Cemalovic N, Scoccimarro A, Arslan A, Fraser R, Kanter M, Caputo N. Human factors in the emergency department: Is physician perception of time to intubation and desaturation rate accurate? Emergency medicine Australasia : EMA. 28(3):295-9. 2016. [pubmed]