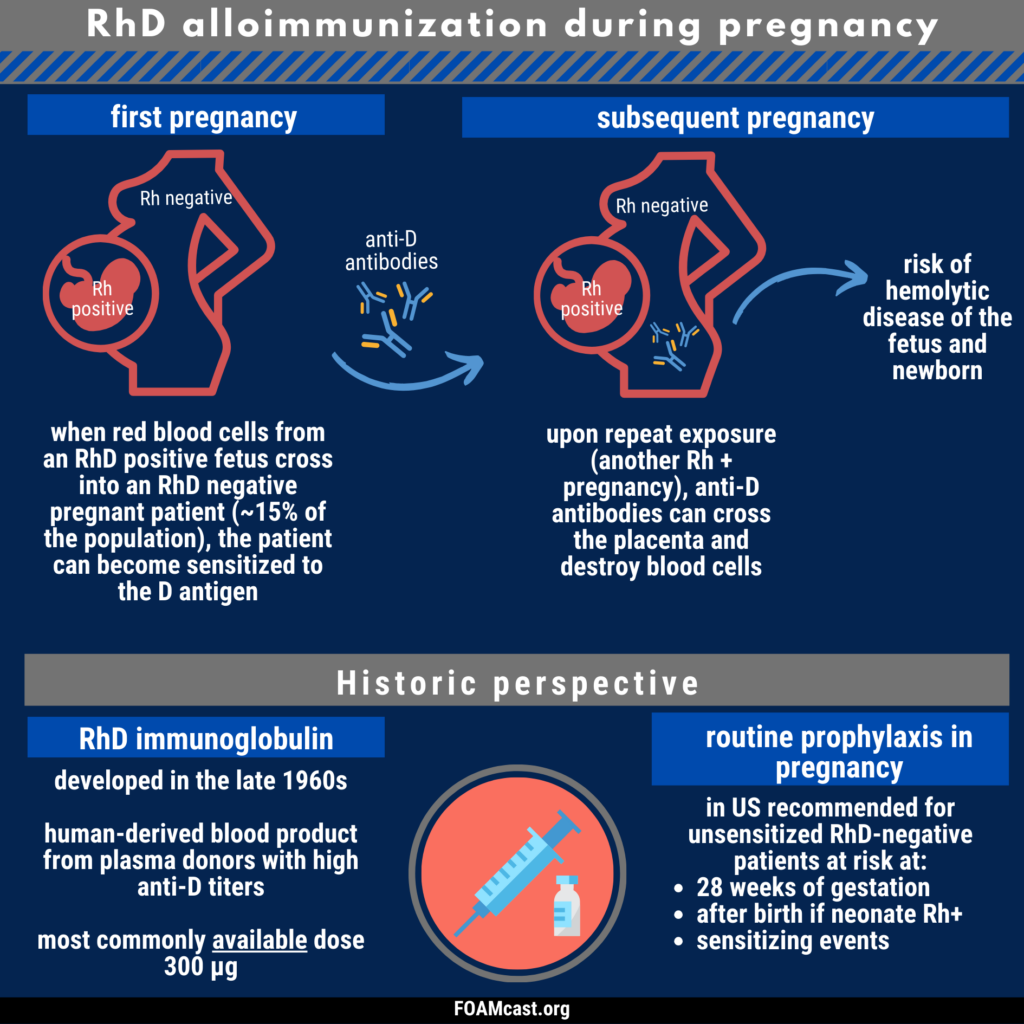
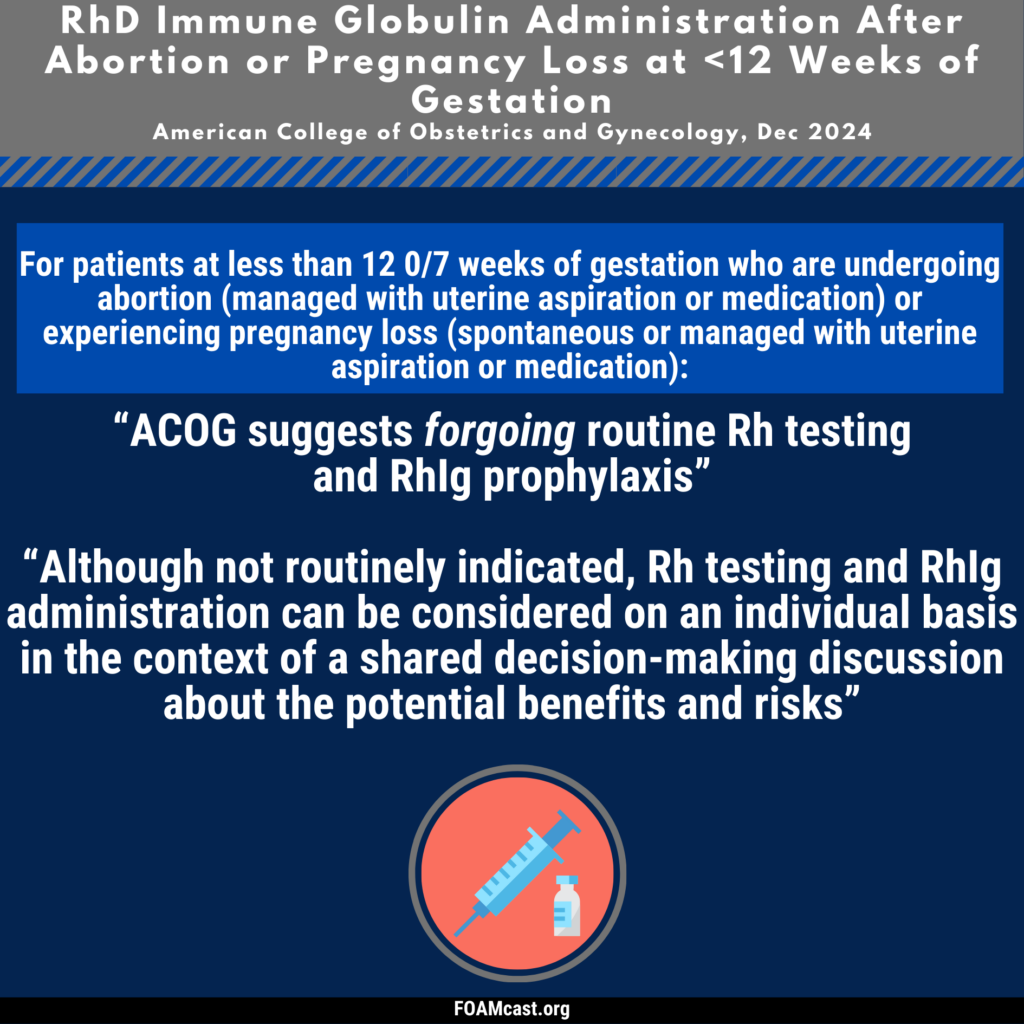
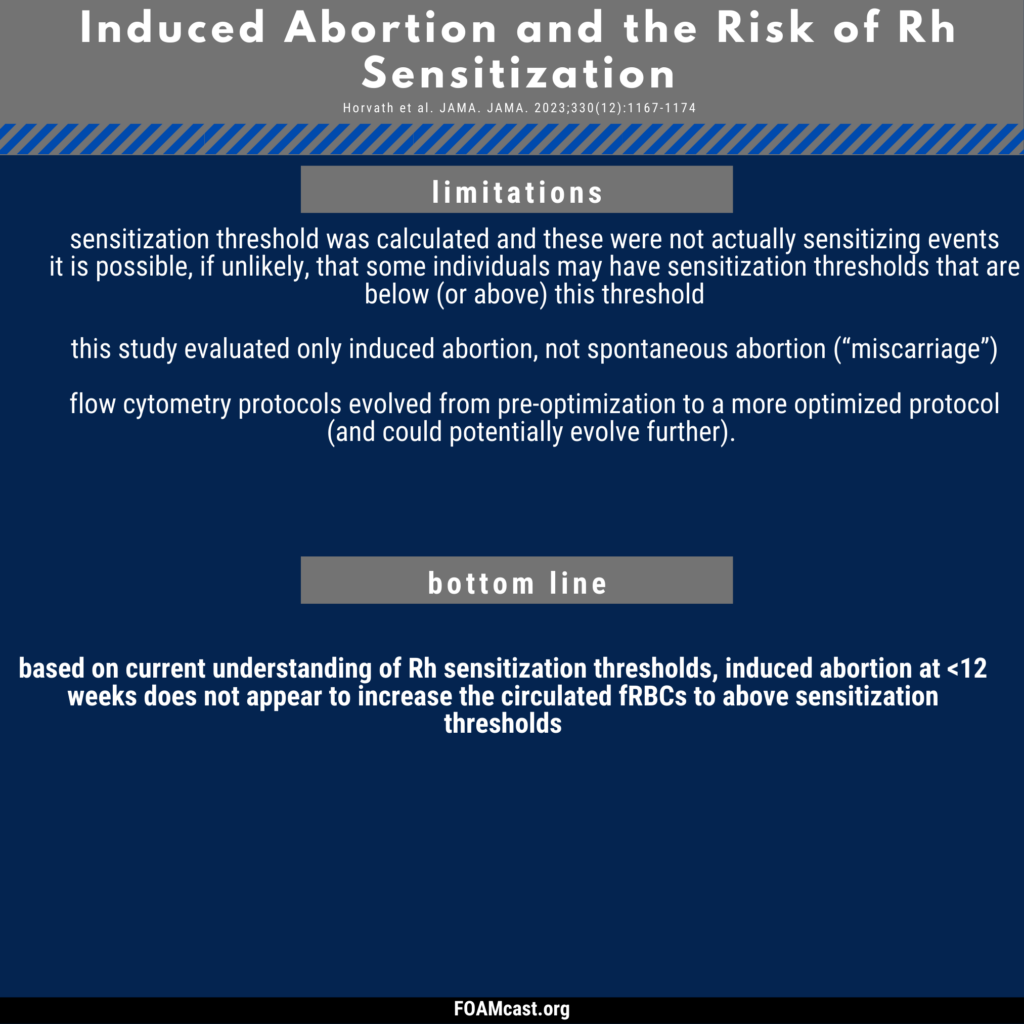
Historically, care of patients in the emergency department (ED) in the first trimester with any kind of abortion (e.g. spontaneous “miscarriage”) underwent blood type and Rh testing followed by RhD immunoglobulin prophylaxis if Rh+. However, many guidelines now recommend foregoing this process in first trimester abortion (spontaneous or induced). In this episode, we dive into the evidence behind these varying recommendations.
We are at SMACC in Dublin – thanks to the Rosh Review, an excellent board review question bank.
Do We Make Saves?
Dr. Mervyn Singer “Is Survival Predetermined in the Critically Ill?”
Many critical care studies are negative, but in some cases this may be because critically ill patients don’t have a uniform prognosis.
Dr. Singer argues that some people may be “destined to die” and some may be “destined to live.” Interventions may be harmful or futile in one group but beneficial in the other. For example, Dr. Singer references the CORTICUS trial of steroids in septic shock [1]. This was a negative trial. Dr. Singer asserts that some evidence (of not great quality), purports that the sickest patients could benefit from steroids, while this same intervention could be deleterious in the healthier ones.
Problem: many of the studies that go back and re-analyze these groups looking at the sickest or least sick patients? They perform subgroup analyses, a form of data dredging that must be taken with a huge grain of salt.
Favorite Pearls
Dr. Suzanne Mason – “Acute Care of the Elderly”
Hospital admission may not benefit geriatric patients – interdisciplinary interventions involving nurses, consultants, pharmacists, physical therapy may be best.
If there is a single, free intervention that providers can do it’s assessing for polypharmacy. Polypharmacy in the elderly is a huge problem. Check the patient’s medication list and beware adding new medications that may not be absolutely necessary.
Dr. Victoria Brazil – “So You Think You’re a Resuscitationist?”
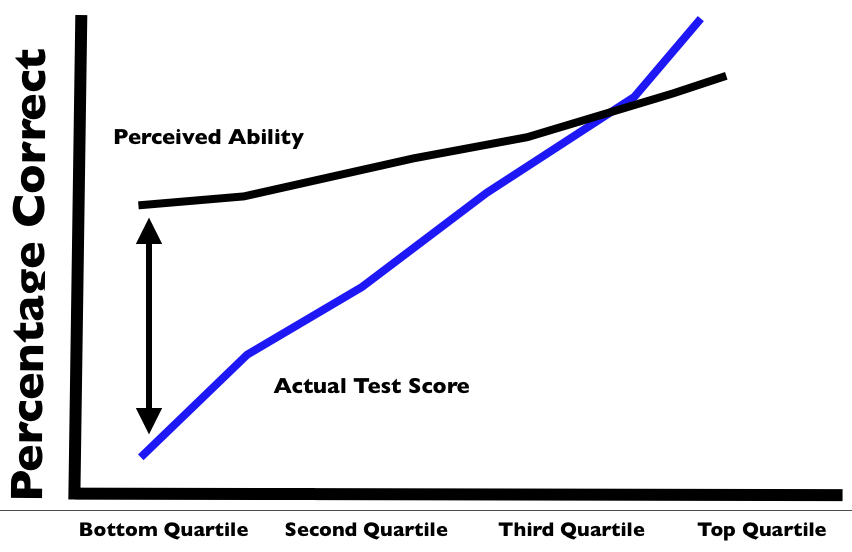
The Dunning-Kruger effect is real in medicine and this is why we MUST have and provide feedback. A review of the Dunning-Kruger effect can be found here. Essentially, people tend to overestimate what they know (i.e. overly confident in their knowledge). The exception? Masters tend to underestimate their knowledge.
Our perception of reality is very skewed so, again, feedback is crucial. For example, Cemalovic and colleagues found that intubators underestimated the time they took to intubate: they estimated 23.5 seconds on average vs the 45.5 seconds intubation actually took. Additionally, they thought 13% of their patients desaturated during intubation but 23% actually desaturated [2].
Also, there was an excellent tribute to the late Dr. John Hinds, a reminder that by living profoundly, you can impact people across the world.
References
Sprung CL, Annane D, Keh D et al. Hydrocortisone Therapy for Patients with Septic Shock. N Engl J Med. 358(2):111-124. 2008. [article]
Cemalovic N, Scoccimarro A, Arslan A, Fraser R, Kanter M, Caputo N. Human factors in the emergency department: Is physician perception of time to intubation and desaturation rate accurate? Emergency medicine Australasia : EMA. 28(3):295-9. 2016. [pubmed]
Life in the Fast Lane Research and Reviews (LITFL R&R) #121 featured a section on the new American Gastroenterology Association (AGA) guidelines on diverticulitis. The game changer? Antibiotics aren’t a requirement in select patients with uncomplicated acute diverticulitis [1].
The guidelines based this recommendation on two studies, previously covered by Dr. Ryan Radecki on Emergency Medicine literature of note over the past 3 years. This post details a prospective observational study on antibiotics for acute diverticulitis [2]. In another post, Dr. Radecki discusses an RCT of antibiotics (ABX) vs IV fluids only.
623 patients with an episode with a short history and with clinical signs of diverticulitis, with fever (>38 Celsius) and inflammatory parameters, verified by computed tomography (CT), and without any sign of complications (fistula, perforation, abscess) or signs of sepsis
Randomized to IVF only or IVF + antibiotics
Primary Outcome – 6 patients (1.9%) developed complications in the no ABX arm vs 3 patients (1.0%) in the ABX arm (not statistically significant). Overall study complication rate was 1.4% [3].
Of note, since 2012, the Cochrane Review suggests that antibiotics may not be necessary in uncomplicated appendicitis [4].
A note on LITFL R&R – every week this blog post features 5-10 high yield articles, culled from contributors across the globe from all kinds of literature – pediatrics, critical care, emergency medicine, etc. It is difficult to keep up with the literature and some have estimated that the number needed to read (NNR) to of 20-200, depending on the journal [5]. Those looking for high yield articles may find their time well spent focused on this cherry picked selection of articles.
Core Content
We delve into core content on diverticula and clostridium difficile using Rosen’s Medicine (8e), Chapters 31, 173 and Tintinalli’s Emergency Medicine: A Comprehensive Study Guide(7e) Chapters 76, 85.
Diverticulosis
Diverticula are small herniations through the wall of the colon (small outpouchings). Often this is asymptomatic, identified incidentally on imaging or colonoscopy. Most common cause of lower gastrointestinal bleeding (LGIB) in adults in the U.S.
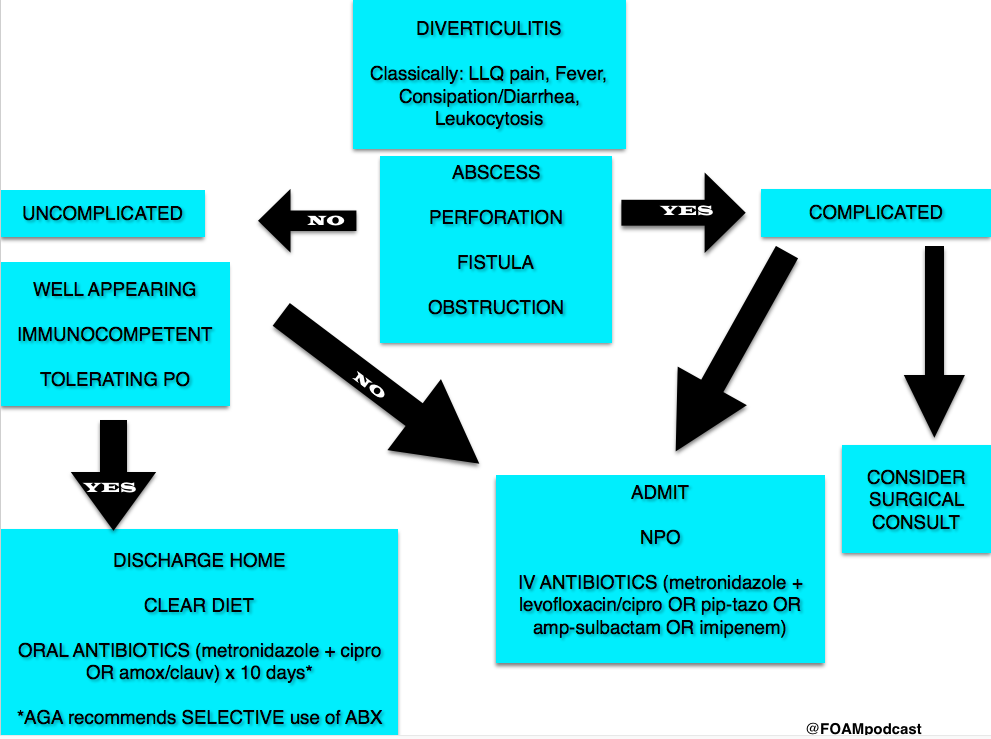
Diverticulitis
Diverticulitis Algorithm
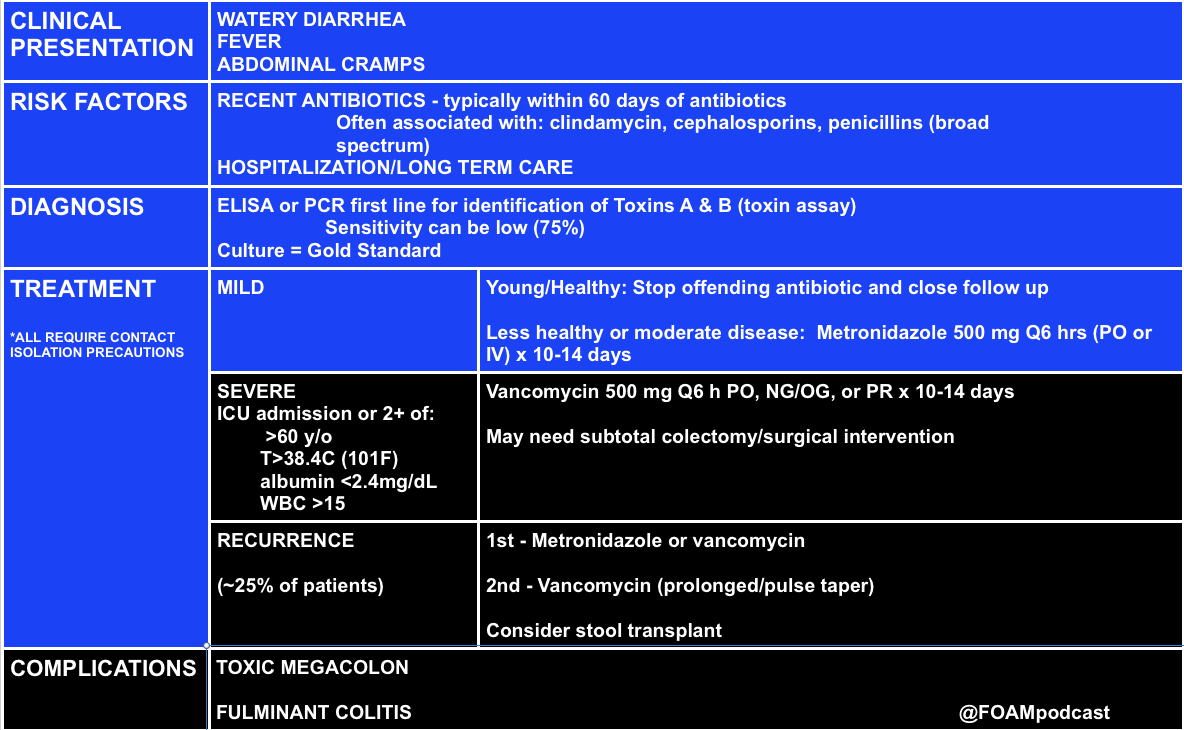
Clostridium Difficile (c. diff)
Note on testing – asymptomatic carriage rates of c.diff vary based on the population but may be between 3-50%. Textbooks quote a 3% carriage rate in newborns and rates of 20%-50% in hospitals and long term care facilities, respectively [10,11].
C. diff historically has a unique odor, refrains of “it smells like c. diff” echo in the halls. Yet this does not perform very well, essentially a coin flip based on a 2013 study by Rao and colleagues. They had 18 nurses smell 10 stool samples (5 c. diff positive and 5 c. diff neg) and found the median percent correct identification of c. diff positive vs negative was 45% [6].
Rosh Review Questions
Question 1. [polldaddy poll=9330955]
Question 2.A 75-year-old woman presents with several days of voluminous watery stools. She was discharged from the hospital one week ago following treatment for pneumonia. Stool studies reveal C. difficile toxin. [polldaddy poll=9333580]
Answers:
C. Patients who present with uncomplicated diverticulitis should be treated with oral antibiotics for 7-10 days. Diverticulitis is an inflammation of the diverticulum in the large intestine. In uncomplicated cases of diverticulitis, patients present with abdominal pain typically in the left lower quadrant with tenderness to palpation in the same area. Patients should not have peritoneal signs or masses on examination. Complicated diverticulitis is defined as the presence of either extensive inflammation or complications such as abscess, peritonitis or obstruction. Patients with uncomplicated diverticulitis can be empirically treated with antibiotics (typically as an outpatient) for 7-10 days. Patients with uncomplicated diverticulitis typically do not require CT imaging (A). Patients with complicated diverticulitis should be treated with intravenous antibiotics (B) and admitted to the hospital. Ultrasound (D) has shown promise in diagnosing diverticulitis but CT is the imaging modality of choice.
C.C. difficile infection is caused by a spore-forming obligate anaerobic bacillus that causes a spectrum of disease ranging from diarrhea to pseudomembranous colitis. C. difficile is the most common cause of infectious diarrhea in hospitalized patients in the United States. Risk factors for infection include broad-spectrum antibiotic use, particularly clindamycin, though other antibiotics have also been implicated. Additional risk factors include prolonged hospitalization, advanced age, and underlying comorbidities. The spectrum of clinical manifestations includes frequent watery stools to a more toxic clinical presentation with profuse stools (up to 20-30 per day), crampy abdominal pain, fever, leukocytosis, and hypovolemia. C. difficile colitis should be suspected in patients who develop diarrhea while taking or after recent cessation of antibiotics, or among recently discharged patients who develop diarrhea. Diagnosis is confirmed by identification of C.difficile toxin in the stool. Colonoscopy, while not usually necessary for diagnosis, reveals characteristic yellowish plaques in the intestinal lumen, confirming pseudomembranous colitis. Treatment for C. difficile infection depends on disease severity. Previously healthy patients with very mild symptoms may be managed by cessation of the offending antibiotic and close clinical monitoring. Oral metronidazole, 500 mg po every 6 hours for 10-14 days is the treatment for moderately severe colitis. Severely ill patients should be hospitalized and treated with oral vancomycin, 125 mg po every 6 hours for 10-14 days.
Isacson D, Thorisson A, Andreasson K, Nikberg M, Smedh K, Chabok A. Outpatient, non-antibiotic management in acute uncomplicated diverticulitis: a prospective study. Int J Colorectal Dis. 2015;30(9):1229–1234. doi:10.1007/s00384-015-2258-y.
Chabok A, Phlman L, Hjern F, Haapaniemi S, Smedh K. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br J Surg. 2012;99(4):532–539. doi:10.1002/bjs.8688.
Shabanzadeh DM1, Wille-Jørgensen P.Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev. 2012 Nov 14;11:CD009092. doi: 10.1002/14651858.CD009092.pub2.
McKibbon KA, Wilczynski NL, Haynes RB. What do evidence-based secondary journals tell us about the publication of clinically important articles in primary care journals? BMC Med. 2004;2:33.
Rao K, Berland D, Young C, Walk ST, Newton DW. The Nose Knows Not: Poor Predictive Value of Stool Sample Odor for Detection of Clostridium difficile. Clinical Infectious Diseases. 56(4):615-616. 2012.
“Chapter 85: Diverticulitis.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e.New York, NY: McGraw-Hill; 2011. p 578-581.
“Disorders of the Large Intestine.” Rosen’s Emergency Medicine, 8th e. p 1261-1275.
“Gastrointestinal Bleeding.” Rosen’s Emergency Medicine, 8th e. p 248-253.
“Infectious Diarrheal Disease and Dehydration.” Rosen’s Emergency Medicine, 8th ep 2188-2204.
“Chapter 76: Disorders Presenting Primarily with Diarrhea.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e.New York, NY: McGraw-Hill; 2011. p 534-535
We cover two bits of FOAM, one from Emergency Medicine Literature of note on the use of meclizine for vertigo and an EMcrit episode on the HiNTs exam.
Emergency Medicine Literature of Note – Dr. Ryan Radecki – Treating what you believe is peripheral vertigo?Using meclizine? So are most people.But this is not an evidence based practice. While meclizine is Rosen approved, Tintinalli recommends transdermal scopolamine as the first line treatment [1,2]. Following a recent recall of meclizine (oddly because iron bottles contained meclizine instead of iron), Dr. Radecki probes into why we use meclizine for vertigo.
Meclizine is an anti-histamine and has been thought to have anti-emetic properties.
A 1968 paper compared 16 anti-emetics/combinations and did NOT conclude that meclizine was the best. In fact, scopolamine and amphetamine performed best. Promethazine (phenergan) is also a good choice based on this paper [3].
EMcrit – Dr. Scott Weingart – The HiNTs exam has taken off, particularly in the FOAM world, as a means of disguising between central and peripheral causes of vertigo. In 2010, an EMcrit episode popularized this in the FOAM world. See this video demonstrating the HiNTs exam.
Head Impulse – rapid head rotation by the examiner with the subject’s vision fixed on an object (i.e. examiner’s nose). The examiner rapidly rotates the head towards midline and the patient’s eyes should remain fixed on the target.
Abnormal (loss of fixation on target and movement of eyes away from target followed by correct saccade as patient fixates on target) = peripheral (vestibulo-ocular reflex impaired)
Normal = central
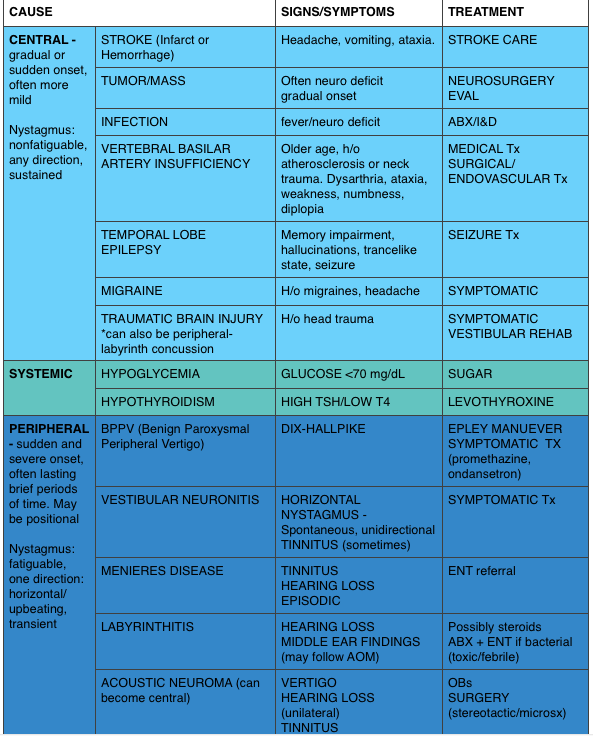
Nystagmus
Horizontal nystagmus with a unidirectional fast phase (away from affected side) = probably peripheral
Patients with horizontal nystagmus may have central pathology but may have direction-changing nystagmus (i.e. fast phase beating in one direction when looking to right and the opposite direction when looking left).
Vertical or nystagmus = central pathology
Test of Skew Patients should fixate on a target while the provider alternately covers each eye. As the cover is moved from one eye to the other, the uncovered eye must correct for the misalignment and will look up or down to focus back on the target. This slight correction is observed repeatedly as the cover is moved from one eye to the other.
Skew deviation/misalignment = probably central, often in posterior fossa abnormalities
No skew deviation= peripheral
INFARCT – Impulse Normal, Fast-phase Alternating nystagmus, and Refixation on Cover Test
Issues with HiNTs
Can only be performed on patients with continuous vertigo.
External validity is a major issue with HiNTs.
Providers – Of the 4 studies have examined the operating characteristics of HiNTs, none have used emergency providers and instead have examined how the exam performs in the hands of two neuro-ophthalmologists, neuro-otologists, and neurologists with 4 hours of specialized training in the exam. It’s unclear whether HiNTs would be reliable or valid when performed by emergency providers [4-6].
Patients – The patients examined in many of these studies have other indicators of badness on neurologic exam. In one study, patients had to have gait instability and/or truncal ataxia to enroll. Then, 76/101 (76%) of those patients had a central cause. These patients were sick and not the undifferentiated vertiginous patients we see primarily as emergency providers [4-6].
In the words of leading HiNTs expert Dr. Newman-Toker, HiNTs “requires expertise not routinely available in emergency departments.” As such, his team is piloting quantitative video-oculography to aid in diagnosis using HiNTs [7]. An Annals of Emergency Medicine review also warned that HiNTs may not be ready for emergency provider use [9].
We delve into core content on vertigo using Rosen’s Medicine (8e) Chapter 19,and Tintinalli’s Emergency Medicine: A Comprehensive Study Guide(7e) Chapter 164 “Vertigo and Dizziness.”
Vertigo is often characterized by the sensation of spinning and falls into the broad and frustrating category of “dizziness.” Often, when a dizzy patient presents we perseverate on characterizes what the patient means by “dizzy.” However, some argue that this is not an appropriate approach as a study found 50% of patients changed the character of their dizziness when questioned again after 10 minutes [9]. Additionally, the clinical characteristics differentiating peripheral from central causes of vertigo are not entirely reliable. Despite these limitations, it is expected that we are familiar with “classic” presentations.
A 50-year-old man presents with episodic severe vertigo lasting hours, with associated symptoms of unilateral tinnitus, fluctuating low-frequency hearing loss, and aural fullness. [polldaddy poll=9245427]
A 20-year-old woman presents with an acute onset of dizziness. The patient describes the sensation that the room is spinning when she turns her head to the left and it is accompanied by nausea and vomiting. The symptoms resolve with turning her head away from that side. Examination reveals nystagmus elicited by deviating the eyes to the left and no other neurologic findings. [polldaddy poll=9245971]
Answers
1. B. Meniere’s disease is characterized by episodic severe vertigo lasting hours, with associated symptoms of unilateral tinnitus, fluctuating low-frequency hearing loss, and aural fullness. Typical onset is in the fifth decade of life. The cause is uncertain but is speculated to result from allergic, infectious, or autoimmune injury. The histopathologic finding includes endolymphatic hydrops, which is thought to be caused by either overproduction or underresorption of endolymph in the inner ear. Meniere’s disease is a clinical diagnosis mostly based on history. Testing may be obtained to support the diagnosis and rule out other disorders. Audiometry often demonstrates a low-frequency sensorineural hearing loss. An FTA-ABS test may be obtained to rule out syphilis. Electronystagmography (ENG) may demonstrate a unilateral peripheral vestibular weakness on caloric testing. When the diagnosis is uncertain, a brain MRI with contrast is obtained to evaluate for a retrocochlear lesion. The differential diagnosis of Meniere’s disease includes acute labyrinthitis, neurosyphilis, labyrinthine fistula, autoimmune inner ear disease, vestibular neuronitis, and migraine-associated vertigo.The most common cause of peripheral vestibular vertigo in adults is benign paroxysmal positional vertigo (A). BPPV occurs in all age groups but more often between ages 50 and 70 but is not associated with hearing loss and made worse with movement. In a perilymph fistula (C) rapid changes in air pressure (barotrauma), otologic surgery, violent nose blowing or sneezing, head trauma, or chronic ear disease may cause leakage of perilymph fluid from the inner ear into the middle ear and result in episodes of vertigo. Associated signs and symptoms are variable but can include a sudden pop in the ear followed by hearing loss, vertigo, and sometimes tinnitus. Acute vertigo associated with nausea and vomiting (but without neurologic or audiologic symptoms) that originates in the vestibular nerve is known as vestibular neuronitis (D). Vestibular neuronitis can occur spontaneously or can follow viral illness.
2. B. This patient presents with peripheral vertigo most consistent with benign paroxysmal peripheral vertigo (BPPV) and should be treated with an Epley maneuver. Vertigo is defined as the sensation of disorientation in space combined with a sensation of motion. Patients typically describe a “room-spinning” sensation or the feeling of sea sickness. Vertigo can be divided into two types: central and peripheral. Central vertigo are those disorders arising from the central nervous system and include ischemic stroke, vertebrobasilar insufficiency and infectious causes (meningitis, mastoiditis, syphilis). Central vertigo is characterized by longer duration of symptoms, minimal change with position, gradual onset and multidirectional nystagmus. Peripheral vertigo includes BPPV, Meniere’s disease, Labyrinthitis and vestibular neuritis. Peripheral vertigo may have intermittent symptoms (BPPV) or continuous symptoms but should not be associated with other neurologic deficits or changes and should have unidirectional nystagmus. The symptoms in BPPV are elicited by specific movements of the head and relieved by returning the head to a neutral position. The symptoms should be acute in onset and of a short duration. In BPPV, the symptoms are cause by the presence of an otolith in one of the semicircular canals. Although pharmacologic intervention may be necessary in the acute setting with meclizine or benzodiazepines, the best treatment for BPPV is the Epley maneuver. The Epley maneuver is a series of positions that the clinician takes the patient through that leads to expulsion of the otolith from the semicircular canal and relief of symptoms. Imaging with a non-contrast head CT (C) is not indicated in peripheral vertigo of any cause as the patient’s pathology is in the inner ear and not the brain. If a central cause is suspected, MRI of the brain (A) is the best test for diagnosis as the causative lesion will likely be in the posterior fossa, which is not seen well on CT scan. Steroid treatment (D) is the indicated management for vestibular neuritis but does not play a role in the treatment of BPPV.
References:
Chang AK, Olshaker AS. Dizziness and Vertigo. In: Marx JA, Hockberger RS, Walls RM eds. Rosen’s Emergency Medicine, 8th e.
Goldman B. Chapter 164. Vertigo and Dizziness. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds.Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011.
Cohn B. Can Bedside Oculomotor (HINTS) Testing Differentiate Central From Peripheral Causes of Vertigo? Annals of Emergency Medicine. 64(3):265-268. 2014.
Strupp M, Zingler VC, Arbusow V et al. Methylprednisolone, Valacyclovir, or the Combination for Vestibular Neuritis. N Engl J Med. 351(4):354-361. 2004.
Jane Brody wrote an article, “What Comes After the Heimlich Maneuver” that ran in the NY Times and stirred up a ruckus on Twitter. This is a reasonable article on choking and details the limitations of the Heimlich maneuver. Unfortunately, the article ends instructing the layperson do to a cricothyrotomy (cric) with a sharp knife and “something like a straw or casing of a ballpoint pen (first remove the ink cartridge). “
Dr. Seth Trueger (@MDaware) wrote a post, Bad Idea Jeans, discouraging this practice saying that deciding which patient needs a cric is one of the more difficult but more important parts of this procedure.
On another note, our friend Dr. Andy Neill has found that medical students are able to perform crics with Papermate pens on cadavers [1]. However, it appears that most pens may not be suitable [2]. Further, while medical students are nearly lay people, we do not think this the cric should be within the domain of lay people (especially without patients already declared dead and preserved).
Cricothyrotomies – In reality, this is a bloody procedures that should only be done by those with proper training when the airway cannot be otherwise secured. The actual procedure has been detailed by those far smarter and with more experience than the FOAMcast crew. We recommend checking out Dr. Scott Weingart’s compilation of resources here.
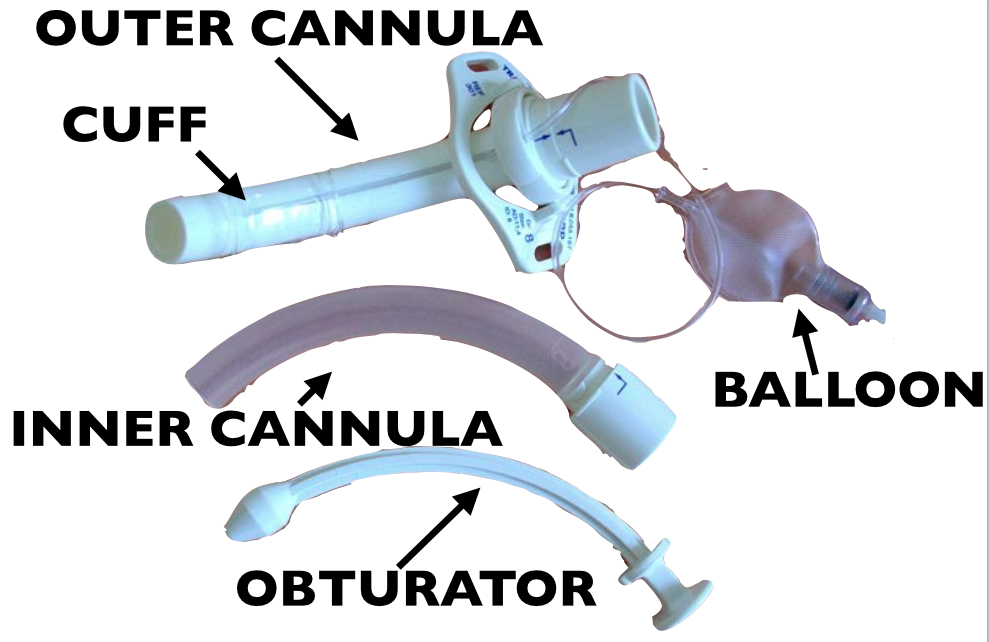
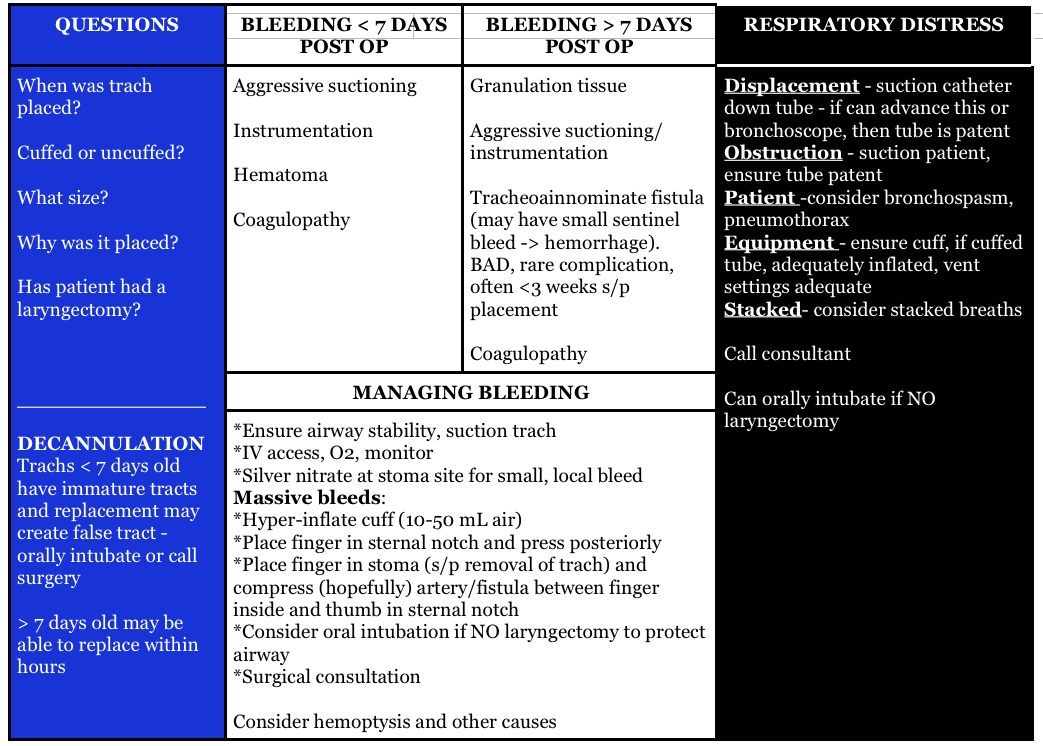
Question 1. A 72-year-old man who is 1 week out from an ischemic stroke presents with respiratory distress. He had a tracheostomy placed 6 days ago for sudden respiratory failure. The patient is hypoxic and tachypneic on presentation with minimal breath sounds bilaterally. There is no subcutaneous air around the stoma.[polldaddy poll=9110296]
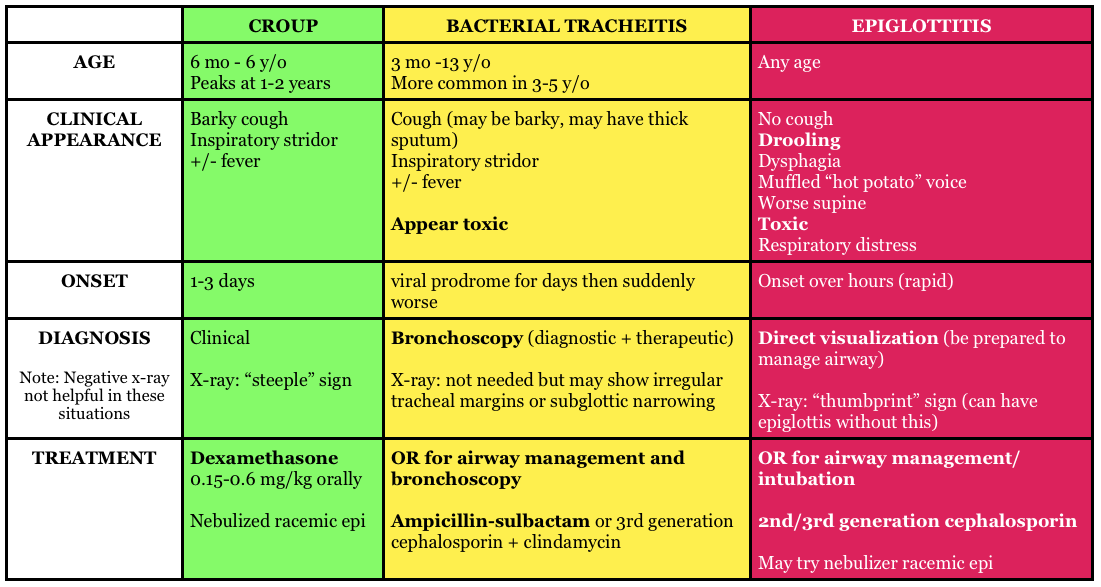
Question 2. A 3-year-old boy presents in severe respiratory distress. His mother informs you that he has been ill for the last 5 days, initially with a low-grade fever and “barky cough.” He was seen at an urgent care facility 4 days ago and given a “breathing treatment” and discharged on steroids. He has become progressively worse despite compliance with the steroid regimen, which prompted his mother to call an ambulance this morning. He is otherwise healthy and up-to-date on his immunizations. On examination, the child is toxic in appearance and febrile. His oropharynx is clear. You hear both inspiratory and expiratory stridor. [polldaddy poll=9110301]
Answers
1.The patient’s presentation is concerning for airway obstruction and the first step in management is suctioning of the tracheostomy tube. Tracheostomy tubes are placed for long-term mechanical ventilation in patients with anticipated prolonged or permanent respiratory failure. The two most common complications are obstruction and dislodgement. Sudden onset of respiratory failure often indicates mucous plugging or equipment failure. Suctioning of the tracheostomy is a simple procedure that may quickly relieve the patient’s symptoms. 2 to 3 ml of normal saline should be instilled into the tube followed by suctioning. Patients with slower decline in respiratory status may have a worsening of their underlying pulmonary pathology or may have developed a pulmonary infection. A cricothyrotomy (A) will not lead to effective oxygenation or ventilation as the cricothyroid membrane is above the tracheostomy site. The tracheostomy tube should not be removed and replaced with either an endotracheal tube (C) or a new tracheostomy tube (B) at this time because the tracheostomy tract has not matured at 6 days (this usually occurs at 15-30 days). If equipment failure in the form of a tracheostomy tube malfunction is suspected, the tube should be replaced with fiberoptic visualization to ensure that a false lumen isn’t created.
2.The patient is suffering from acute bacterial tracheitis. Bacterial tracheitis is the result of severe inflammation of the epithelial lining of the trachea leading to thick mucopurulent secretion production. This clinically manifests as viral prodrome with fever, URI symptoms, barky cough and stridor that intensifies and progresses to include a toxic appearing child with signs of airway obstruction, inspiratory and expiratory stridor, cyanosis, and severe respiratory distress. Another clue is that the child has been treated with medications (aerosolized epinephrine and steroids) for croup and has not improved clinically. Bacterial tracheitis is most common in children between the ages of 3 to 5 years. Most patients require orotracheal intubation for respiratory distress and ICU admission. The patient should be started on broad-spectrum intravenous antibiotics. Croup (B) is the most common cause of upper airway distress and obstruction in children between 6 months to 6 years of age with peak incidence at 2 years of age. Croup begins as a prodrome of low-grade fever and URI symptoms and is characterized by a barky cough, inspiratory stridor, and hoarse voice. Children are less toxic in appearance and rarely develop respiratory failure. The mainstays of treatment are steroids and aerosolized epinephrine. Epiglottitis (C) is characterized by abrupt onset of fever and sore throat and children classically present with difficulty in breathing, anxiety, stridor and drooling. This is less common in vaccinated children, such as the patient above and typically occurs in slightly older children. There is generally not a prodrome associated with epiglottitis. Peritonsillar abscess (D) occurs more commonly during adolescence and presents with trismus, unilateral sore throat, fever, tonsillar asymmetry, and uvula deviation away from the affected tonsil. The age of this patient and normal oropharynx examination make this diagnosis very unlikely.
References:
Neill A, Anderson P. Observational cadaveric study of emergency bystander cricothyroidotomy with a ballpoint pen by untrained junior doctors and medical students. Emergency medicine journal : EMJ. 30(4):308-11. 2013. [pubmed]
Owens D, Greenwood B, Galley A, Tomkinson A, Woolley S. Airflow efficacy of ballpoint pen tubes: a consideration for use in bystander cricothyrotomy. Emergency medicine journal : EMJ. 27(4):317-20. 2010. [pubmed]
The paper: The authors took blood samples from 760 healthy pregnant patients at one point during their pregnancy. They propose a continuous increase for a normal d-dimer cut off throughout gestation.
1-12 weeks: n=33, 81% with normal d-dimer
19-21 weeks: n=53, 32% with normal d-dimer
28-36 weeks: n=8, 6% with normal d-dimer
39-40 weeks: 0, 0% normal d-dimer
Postpartum day 2: n=12, 8% with normal d-dimer
Dr. Radecki’s “Take Home:“
Dr. Kline has advocated for the following d-dimer cut offs in pregnancy: 1st trimester 750 ng/mL, 2nd trimester 1000 ng/mL, and 3rd trimester 1250 ng/mL(based on a standard cut-off of 500 ng/mL) and this may be reasonable but is not rooted in robust evidence.
Interestingly, this post was followed by another post covering an article by Hutchinson et al from Am J Roentgenol showing that of 174 CTPAs initially read as positive, 45 were read as negative by chest radiologist upon blinded retrospective review. That means 25.9% of this cohort diagnosed with PE apparently had negative CT scans.
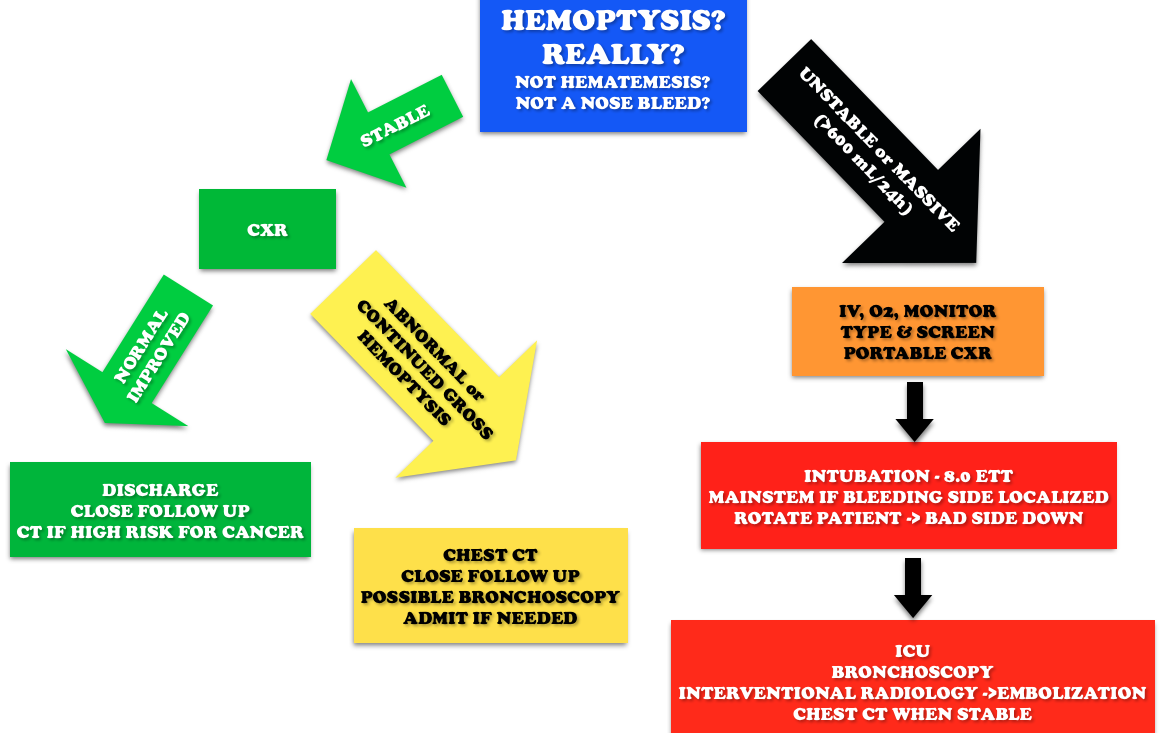
Core Content – Hemoptysis
Tintinalli (7e) Chapter 66; Rosen’s Emergency Medicine (8e) Chapter 24
Etiology: Most common causes are bronchitis (often blood tinged sputum), infection (abscess, pneumonia, tuberculosis), neoplasm (lung cancer). Other causes include iatrogenic causes (bronchoscopy, biopsy, aspirated foreign body), anticoagulation, and autoimmune diseases such as granulomatous polyangiitis (Wegener’s), lupus, and Goodpasture’s.
Question 1. A 50-year-old man, nonsmoker, presents to the ED with a 2-day history of cough now associated with frank hemoptysis. He denies any constitutional symptoms. Vital signs are BP 125/70, HR 80, RR 16, and pulse oximetry is 98% on room air. On exam, his lung fields are clear; the remainder of the exam is unremarkable. A chest radiograph is performed, which is normal. [polldaddy poll=9039260]
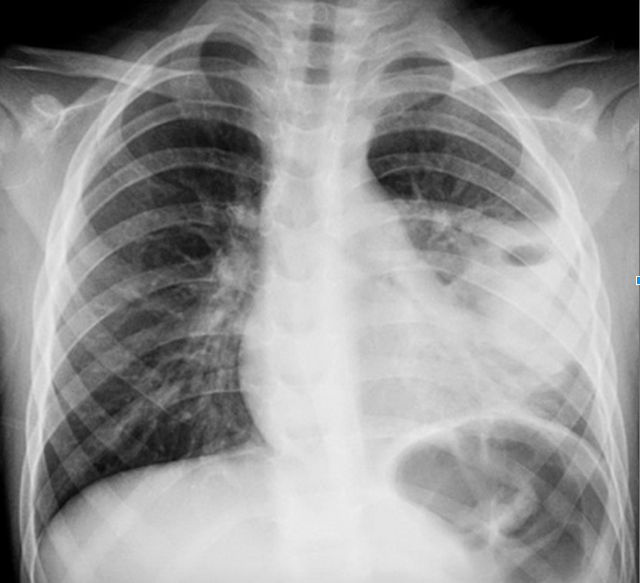
Question 2. A 55-year-old man, smoker, presents to the ED with hemoptysis and dyspnea for 4 weeks. His VS are T 37°C, BP 146/76 mm Hg, HR 85 bpm, RR 20 per minute, and oxygen saturation 96% on RA. His lung exam reveals distant breath sounds on the left side. His chest X-ray is shown below. [polldaddy poll=9039262]
Rosh Review
Answers
1.C. The patient is hemodynamically stable with a normal chest radiograph, so he does not require ICU admission (A). Patients with massive hemoptysis require ICU admission. The decision to perform a bronchoscopy (B) in this patient will be left up to the pulmonologist. Given the overall clinical picture, urgent bronchoscopy is not required in this case. With massive hemoptysis, an emergent bronchoscopy is indicated. Bronchitis (D) typically presents with the abrupt onset of cough with blood-streaked purulent sputum. The patient in the clinical scenario has persistent frank hemoptysis, which mandates further investigation. In a patient who does not smoke, is under the age of 40, and has a normal chest radiograph and scant hemoptysis, treatment for bronchitis can be initiated with outpatient follow-up.
2. B. Although bronchitis (A) is the most common cause of hemoptysis (responsible for 15%-30% of cases), patients present with cough as the dominant symptom and have abnormal lung exams and normal chest x-rays. The cough may be productive of sputum. The diagnosis of pneumonia (C) requires focal findings on physical exam or infiltrates on radiographic imaging and is typically accompanied by a fever. Patients with lung cancer are at increased risk for pulmonary embolism (D). This patient’s Wells score is 2 (one point each for hemoptysis and malignancy), which makes the likelihood of PE 16% in an ED population. Given the lung mass seen on chest x-ray, lung cancer is more likely than PE.
This week we cover a post from Dr. Rory Spiegel, author of EMnerd, on initial nonoperative management of acute appendicitis based on an article by Salminen et al in JAMA 2015.
530 patients with CT confirmed acute, uncomplicated appendicitis were randomized to operative intervention (n=273 receiving open laparotomies) or non-operative intervention (n=257 receiving antibiotics).
27.3% (n=70, CI 22-33.2%) of patients who received medical management (ertapenem x 3 days then 5 days of levofloxacin) had an appendectomy by the 1 year mark
7 patients (2.7%) in medical management group had complicated appendicitis at one year, 0 had abscesses
45 patients (20.5%) in the operative group had surgical complications
This is a non-inferiority study where the intent is to demonstrate that an experimental treatment (antibiotics alone) is not substantially worse than a control treatment (immediate surgery). The authors set the non-inferiority margin at 24%, which means that a failure rate (appendectomy by 1 year) >24% would render medical management inferior.
Authors Conclusion: “Among patients with CT-proven, uncomplicated appendicitis, antibiotic treatment did not meet the prespecified criterion for noninferiority compared with appendectomy.”
Spiegel’s Conclusion: “there is a great deal to be determined before this non-invasive strategy can be considered mainstream practice…in what was once considered an exclusively surgical disease, the majority of patients can effectively be managed conservatively. Despite not meeting their own high standards for non-inferiority, the authors demonstrated that for most patients with acute appendicitis, when treated conservatively with antibiotics we can avoid surgical intervention without complications of delays to definitive care.”
More FOAM on non-operative treatment of appendicitis: The SGEM
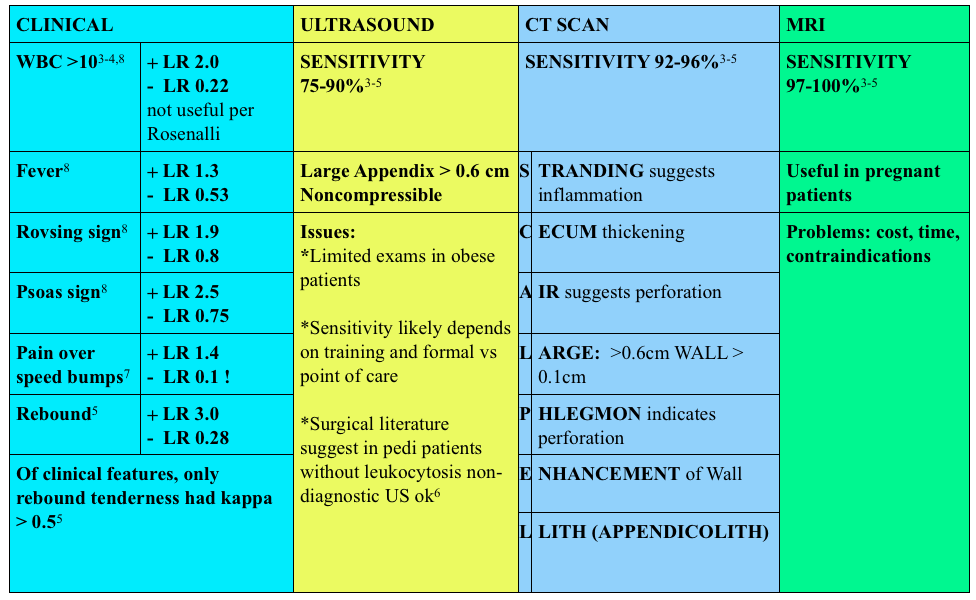
Use of contrast enhanced CT scans controversial. Rosenalli and the American College of radiology concur that oral contrast is probably not needed but does increase the emergency department length of stay [3-5].
Treatment:
Surgical consult
Antibiotics:
Broad spectrum beta-lactams: ampicillin-sulbactam 3g IV (75 mg/kg IV in peds) piperacillin-tazobactam 4.5g IV, cefoxitin 2g IV (40 mg/kg IV in peds) OR metronidazole 500 mg IV + ciprofloxacin 400 mg IV
Other things to consider in special populations in right lower quadrant:
1. A 22-year-old man presents with abdominal pain followed by vomiting for 1 day. His examination is significant for right lower quadrant tenderness to palpation. He has a negative Rovsing sign. [polldaddy poll=9026936]
2. A 22-year-old woman presents with lower abdominal pain and vaginal discharge. She is sexually active with men with inconsistent barrier protection. Her vitals are normal other than temperature of 101°F. On examination, there is yellow cervical discharge, no cervical motion tenderness, but uterine and left adnexal tenderness. An ultrasound does not show any evidence of tubo-ovarian abscess. [polldaddy poll=9026939]
Answers.
1. B. Sensitivity or the true positive rate measures the proportion of actual positives that are correctly identified as such. It is determined by dividing the number of true positives of the test by the number of true positives + false negatives. Tests with a high sensitivity are good for ruling out disease as the test has very few false negatives. A test with high sensitivity is advantageous as a screening tool as it misses very few people with the disease. The onset of pain before vomiting has been found to be as high as 100% sensitive in diagnosing acute appendicitis.Rovsing’s sign (D) (indirect tenderness) describes pain felt in the right lower quadrant upon palpation of the left lower quadrant. This sign signifies the presence of peritoneal irritation and has a sensitivity of 58%. Right lower quadrant pain (C) has a sensitivity of 81% and fever (A) has a sensitivity of 67%.
2.This patient presents with signs and symptoms consistent with pelvic inflammatory disease (PID) and should be treated with ceftriaxone 250 mg IM and 2 weeks of doxycycline. PID is an ascending infection beginning in the cervix and vagina and ascending to the upper genital tract. Neisseria gonorrhoeae and Chlamydia trachomatis are most commonly implicated. It can present with a myriad of symptoms although lower abdominal pain is the most common. Other symptoms include fever, cervical or vaginal discharge and dyspareunia. Pelvic examination reveals cervical motion tenderness (CMT), adnexal tenderness and vaginal or cervical discharge. Inadequately treated PID can lead to tubo-ovarian abscess, chronic dyspareunia and infertility. Due to the variable presentation and serious sequelae, the CDC recommends empiric treatment of all sexually active women who present with pelvic or abdominal pain and have any one of the following: 1) CMT, 2) adnexal tenderness or 3) uterine tenderness. Treatment should cover the most common organisms and typically consists of a third generation cephalosporin (ceftriaxone) and a prolonged course of doxycycline. Patients with systemic manifestations or difficulty tolerating PO should be admitted for management.Ceftriaxone and azithromycin (A) are used in the treatment of cervicitis or urethritis. Clindamycin (C) and metronidazole (D) are used in the treatment of bacterial vaginosis. References:
1.Salminen P, Paajanen H, Rautio T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015;313(23):2340
This week we cover posts from the Wessex ICS site, The Bottom Line, which is an excellent source for breakdown of recent and important trials. This site is great for reviews of high impact trials in critical care. We cover their post on a systematic review of peripheral pressor complications and then we delve into a recent prospective trial by Cardenas-Garcia and colleagues that came up at SMACC.
Systematic review of the literature 1946-Jan 2014 (does not include most recent trial)
Outcome – local tissue injury or extravasation: 325 separate events, 318/325 peripheral pressors
Signal that distal lines are not ideal for running pressors: 204 events (local tissue injury) were distal to the antecubital fossa/popliteal fossa (90% of events)
Signal that duration of pressors running peripherally may impact likelihood of adverse event. Increasing number of events were reported at the 6-12 hour mark (n=9) then 12-24 hour (n=18) and then almost all >24 hour
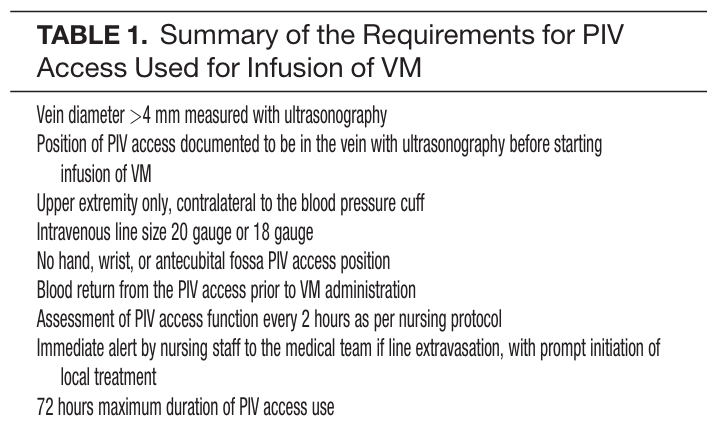
ICU fellows and attendings determined if peripheral pressors were warranted and then initiated the following protocol:
Vein diameter >4 mm measured with ultrasonography and PIV confirmed with US before pressors started
Upper extremity only, contralateral to the blood pressure cuff
IV size 20 gauge or 18 gauge
No hand, wrist, or antecubital fossa PIV access position
Blood return from the PIV access prior to VM administration
Assessment of PIV access function q 2h as per nursing protocol
Immediate alert by nursing staff to the medical team if line extravasation, with prompt initiation of local treatment
72 hours maximum duration of PIV access use
N=734 patients
19/783 peripheral vasopressor administrations with infiltration of site (2%) with no events of local tissue injury
The take home: If a patient needs vasopressors, you can start them through a good, proximal peripheral IV. Sometimes patient or situation factors delay central lines, this doesn’t mean it needs to delay patient’s therapy. Know what to do in the event of infiltration (see this EMCrit post).
Core Content
Tintinalli (7e) Chapter 24
Panchal et al – Phenylephrine bolus dosing in peri-intubation period
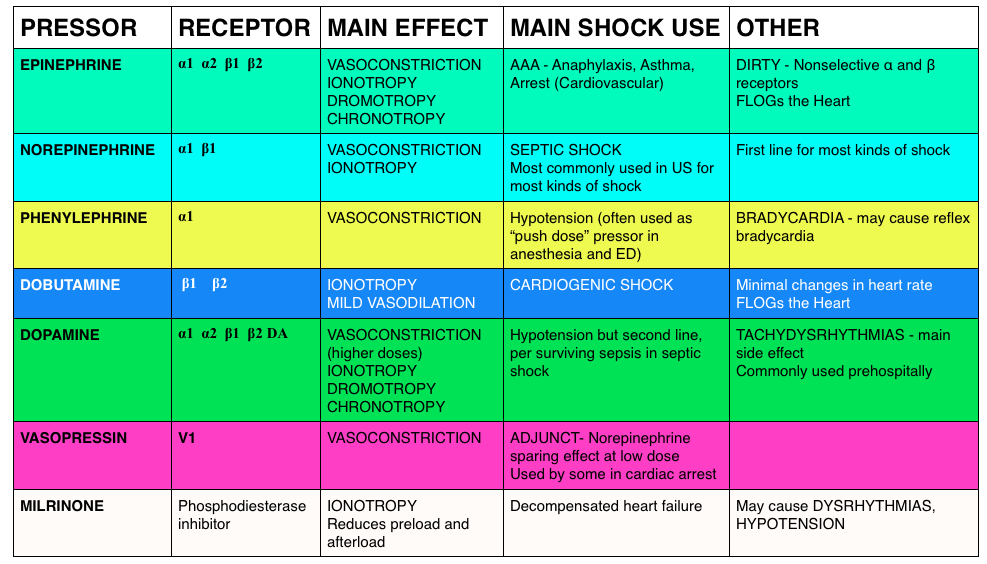
Answer. C. Norepinephrine is considered the vasopressor of choice for treatment of septic shock. Norepinephrine acts primarily as an α-adrenergic agonist, causing vasoconstriction that results in an increase in blood pressure. It also has β-adrenergic properties, which causes an increase in cardiac output and heart rate. The combination of α-adrenergic and β-adrenergic properties benefits patients who have septic shock. Norepinephrine also has a short duration of action, which allows for rapid adjustment of dosing in response to changes in a patient’s hemodynamic status. Dopamine (A) was once widely used in the treatment of septic shock, but studies have shown that it has no advantage over norepinephrine and its use is associated with a higher death rate. Epinephrine (B) has both α-adrenergic and β-adrenergic properties and has a greater affinity for alpha- and beta-receptors than norepinephrine. Its use is associated with a higher rate of cardiac dysrhythmias and a decrease in splanchnic blood flow. Phenylephrine (D) is a pure α-adrenergic agent that causes vasoconstriction and impairment of tissue blood flow throughout the body, most notably in the splanchnic circulation.
In a prior FOAMcastini, we covered the updated ACEP tPA clinical policy. As residents, we sought perspectives from experts, the FOAMcast brain trust (Drs. Anand Swaminathan, Ken Milne, Ryan Radecki, and David Newman). We (Jeremy) also interviewed Dr. Jerry Hoffman, faculty at UCLA.
In this interview, Dr. Jerry Hoffman, a public skeptic and author of peer reviewed critiques of tPA provides interesting perspective on more than thrombolysis but on the future of guidelines (referencing this paper) and science in Emergency Medicine.
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The overarching theme to Day 1 at SMACC? Use your team- to keep you in check and for feedback. Our cases and errors are opportunities for reflection. Dr. Cliff Reid reminded us to follow up our patients and outcomes and learn from it all, without letting our egos get in the way. Dr. Simon Carley (St. Emlyn’s) gave a powerful talk on learning from mistakes later in the day; you will definitely want to listen to these when they come out.
The sub theme? Experts don’t need algorithms and tests. But the novices? That’s another story.
Trauma – Weingart. We won’t delve into his thoughts on ATLS here (hint: ATLS isn’t for experts).
Ignore the first automated blood pressure, it’s probably wrong. Get a manual blood pressure.
Giving 3 units of blood in one hour? Prepare for massive transfusion, that means FFP, platelets, everything
If you go down the massive transfusion pathways, give an ampule of calcium every 4-6 units of plasma to combat the transfusion induced hypocalcemia from citrate.
The Shock Index (HR/SBP), isn’t as exciting as we once thought. It may be a guide, but not reliably so.
Pain – Strayer
Analgesia doesn’t = opiates. Think about local analgesia.
Pain as the “5th vital sign” – probably more harmful than helpful [Gussow]
In fact, in 2009, there were
Polypharmacy – Juurlink
Trimethoprim/sulfamethoxazole and ace-inhibitors/angiotensin receptor blockers, used in combination can lead to hyperkalemia and, in some cases, death [Juurlink et al]
Acetaminophen, at just 2 grams/day, can elevate the INR in patients on warfarin [Pinson]. Acetaminophen is still probably the analgesic of choice, but something to be aware of
Sepsis
Lactate is not a measure of tissue hypoxia/anaerobic metabolism [Marik et al]
Too much fluid is not a good thing = iatrogenic salt water drowning [Marik et al]
Patients may need vasopressors. If they do, don’t delay based on central access. Vasopressors are ok through good peripheral lines for a day or so. [Loubani et al, Mayo et al] However, we should probably place the lines when we’re safely able.
Of note, this does require strict protocols. Ex: Mayo study had stringent inclusion criteria