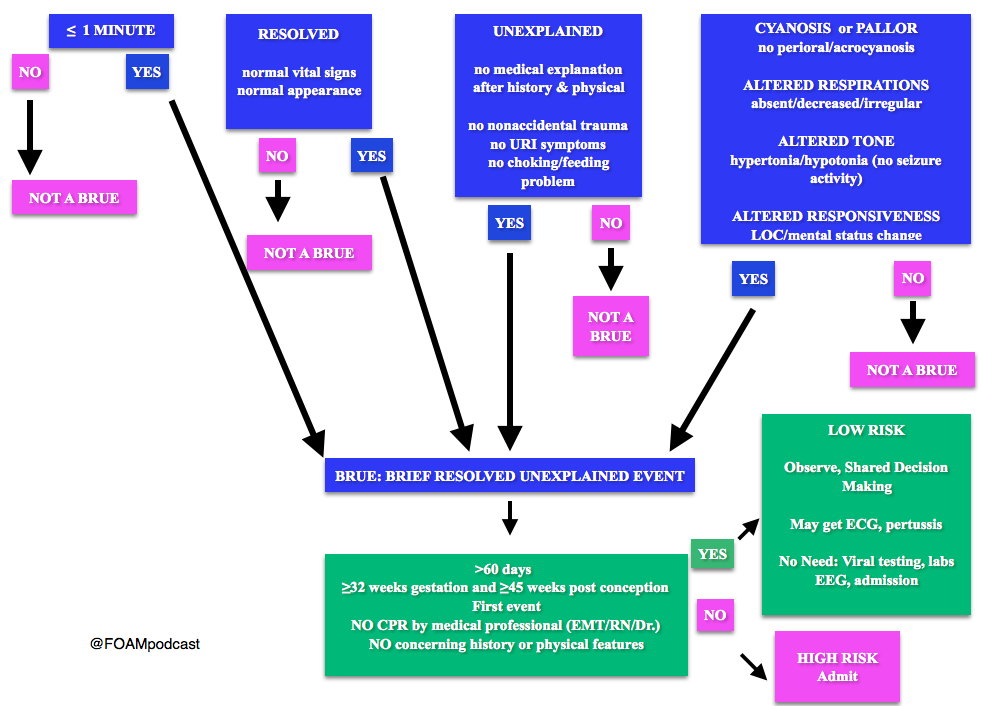
Note: Some have voiced concerns that these guidelines potentially downplay the event. The concern is that the yield of these workups and admissions may be low, but possibly worthwhile. At FOAMcast, we are not qualified to critique these guidelines but there are helpful tables and charts in them to realize that these recommendations really are only for specific events and children AFTER thorough history and physical.
Generously Donated Rosh Review Question
A 6-week-old boy is brought to the emergency room because of cyanosis. He was sleeping comfortably in a supine position right after a feeding when he suddenly choked, became limp and lips turned blue. The mother witnessed the event and blew to the face of the boy. The whole episode lasted for about two minutes. EMS was called and upon arrival at the house, the boy was back to his usual self. At the ER, he boy has normal vital signs with normal physical examination findings.
A. Admit for cardiorespiratory monitoring. The boy in the vignette had an apparent life-threatening event (ALTE) which is not a specific diagnosis but a description of an acute, unexpected episode that is frightening to the caretaker. ALTE includes one or more of the following features: apnea, color change (may be cyanotic, pallid, erythematous or plethoric), marked change in muscle tone (limpness or rigidity) and choking or gagging. A specific cause for ALTE can be identified in over one-half of patients after a careful history, physical examination, and appropriate laboratory evaluation. The remaining cases are considered idiopathic if no cause can be identified after a thorough assessment. Common etiologies for ALTE include gastroesophageal reflux, neurologic problems (such as seizures), and respiratory infection. The history of an ALTE must be taken seriously, even if the infant appears entirely well by the time he or she is evaluated. In-hospital observation with cardiorespiratory monitoring is indicated for infants whose initial evaluation suggests physiologic compromise. Hospital admission may provide important clinical information where additional episodes may be witnessed by medical personnel during the observation period. In addition, serious underlying medical conditions may become apparent. Discharging the patient after reassuring the parents (B) and observing the patient for four hours in the ER (C) are not appropriate management strategies for the infant in the vignette who needs admission for cardiorespiratory monitoring. Requesting for complete blood count (D) is not routinely done in the evaluation of an ALTE and would not aid in the management for the infant in the vignette.
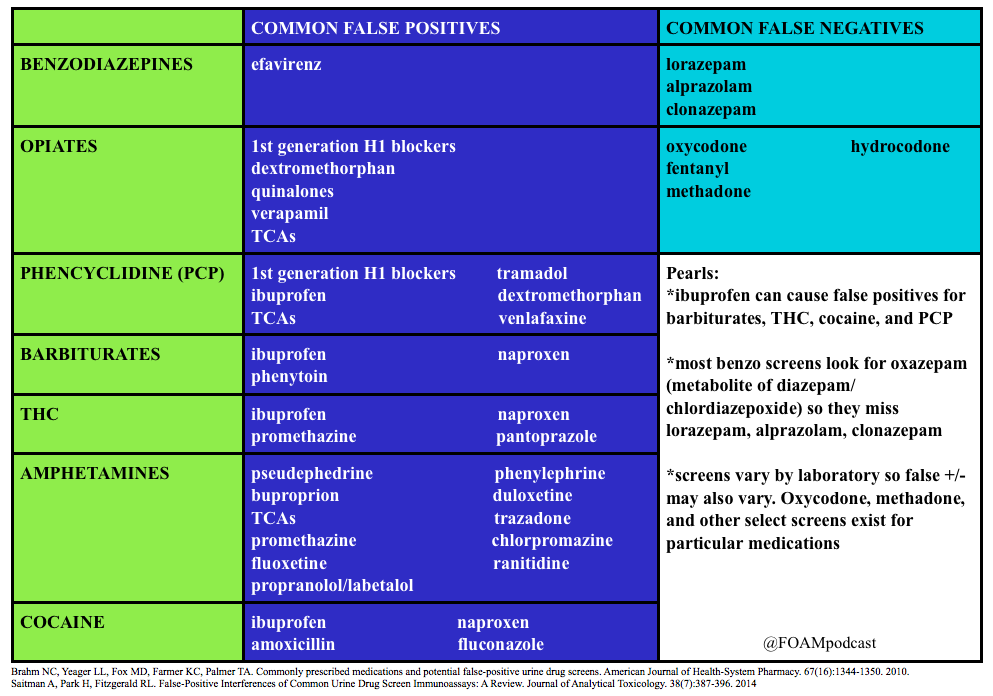
We review a post by Dr. Seth Trueger (@MDaware) on false positives of common medications in the urine drug screen. We delve into posts by Dr. Bryan Hayes (@PharmERToxGuy) on false negatives for benzodiazepines and opioids in the urine drug screen.
Core Content
We delve into core content on cocaine and phencyclidine (PCP) using Rosen’s (8th edition), Chapter 154 and Tintinalli (8th edition)
Cocaine
Cocaine
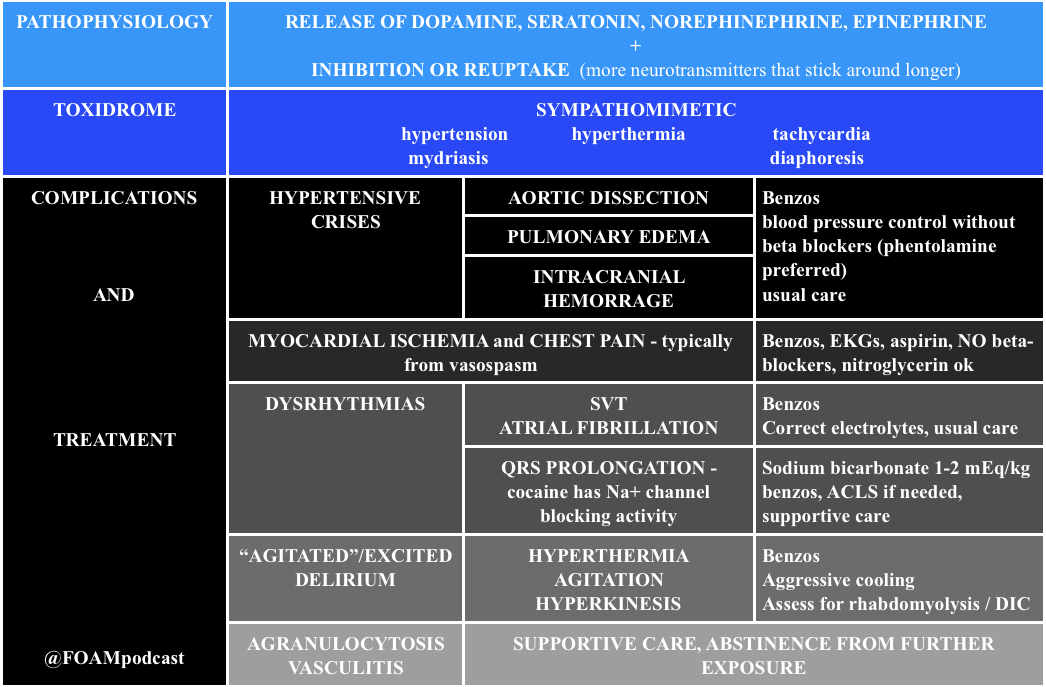
Note: Beta-blockers are contra-indicated in cocaine induced hypertension and chest pain. Much of the ischemia induced by cocaine is thought to be due to vasospasm, predominantly from alpha-1 receptor effects. Beta-blockers block the relaxation provided by beta-2 stimulus on muscles, leaving alpha-1 constricting vessels, “unopposed.” This is largely theoretical/based on canine literature as there are only two human studies on this, (a) 10 humans given propranolol + cocaine with vasospasm and (b) 9 humans given labetalol + cocaine without vasospasm [4,5]. However, recent papers attempting to dispel this teaching don’t quite prove the point. One retrospective chart review looked at cocaine positive urine screens in patients with chest pain and found no worsened troponins. Cocaine stays positive in the urine for 3 days so it is not clear that these were patients presenting with cocaine associated chest pain [6].
Generously Donated Rosh Review Questions
An 18-year-old man is brought to the ED by the police after being found running around a parking lot, screaming at bystanders. He reportedly smoked phencyclidine (PCP) earlier that day. His vital signs are notable for a heart rate of 130 beats per minute and a blood pressure of 150/86 mm Hg. On physical exam, he is diaphoretic, with vertical nystagmus and equal pupils and appears acutely agitated.
A. Administer haloperidol for acute agitation
B. Administer IV fluids for presumed rhabdomyolysis and benzodiazepines for agitation
C. Apply physical restraints; this is adequate treatment for most cases
D. Monitor for traumatic injuries; they are the most common cause of morbidity and mortality with PCP use
E. Urinary acidification to increase PCP elimination
The most common cause of morbidity and mortality in patients with phencyclidine (PCP) intoxication is rhabdomyolysis. Fluid hydration with normal saline is the initial therapy for rhabdomyolysis. Creatinine kinase (CK) should be obtained in patients with PCP intoxication. If abnormal, serial levels should be obtained until a downward trend is noted. Serum creatinine should also be monitored for evidence of renal insufficiency. PCP is a dissociative anesthetic drug that works on the NMDA glutamate receptor. People who abuse PCP can have sensations of euphoria initially, but this can be followed by an emergence reaction that is characterized by dysphoria and psychosis. If initial calming measures such as placing the patient in a calm environment fail and chemical restraints are needed, benzodiazepines are the treatment of choice. Benzodiazepines are also the preferred medication for acute agitation. Haloperidol (A) may cause dysrhythmias and hypotension. It also lowers the seizure threshold and may precipitate PCP-induced movement disorders. PCP is a weak base and its excretion is increased in acidic urine. Physical restraints (C) may be required for patients with PCP intoxication, but they should be used in conjunction with chemical restraints (preferably benzodiazepines). An agitated patient fighting against physical restraints is at risk for worsening rhabdomyolysis, which, if unrecognized, can precipitate cardiac arrest. Traumatic injuries (D)frequently occur in PCP-intoxicated patients; however, rhabdomyolysis with subsequent renal insufficiency is the most common cause of associated morbidity and mortality. Patients with PCP intoxication should be evaluated for suspected trauma, and any injuries should be stabilized and treated. Acidification of the urine (E) can cause a metabolic acidosis, which is potentially harmful and has not demonstrated improved outcomes. For these reasons, urinary acidification is not routinely recommended.
[/toggle]
[/accordion]
2. A 39-year-old woman presents with chest pain and difficulty breathing that began shortly after smoking crack cocaine. Vital signs are BP 190/85 mm Hg, HR 105, RR 18, T 99.1℉. The ECG demonstrates ST segment depression and T wave inversions in the lateral leads.
Diazepam, a benzodiazepine, should be administered to this patient who is hyperadrenergic from cocaine intoxication. Signs and symptoms of cocaine intoxication include, dilated pupils, diaphoresis, tachycardia, hypertension and hyperthermia. Many patients experience euphoria, though some will develop acute psychosis. Benzodiazepines decrease the cocaine-induced hyperadrenergic state. Reduction of sympathetic tone induces coronary and peripheral vasodilation. Coronary artery dilation directly improves myocardial blood flow. Peripheral vasodilation reduces preload and afterload. Reductions in preload and afterload decrease blood pressure and improve myocardial oxygen demand. Several factors, including, excess sympathetic stimulation, dehydration, hyperthermia, and cocaine-induced cardiac sodium channel blockade, may cause patients with cocaine intoxication to develop dysrhythmias. These contributing factors should be treated with benzodiazepines, IV fluid resuscitation and temperature management. In some patients, cocaine-induced cardiac sodium channel blockade may cause wide complex tachycardia that should be treated with sodium bicarbonate. Hyperthermia should be managed aggressively with a target temperature of less than or equal to 102.0℉. Severe agitation, aggression or psychosis should be initially managed with benzodiazepines. Most antipsychotic agents have pronounced anticholinergic side effects. This may worsen dysrhythmias.and decrease sweating, further complicating temperature management
[/toggle]
[/accordion]
Rao R, Hoffman RS. Cocaine and other Sympathomimetics. Rosen’s Emergency Medicine (8e). Chapter 154, 1999-2006.e2
“Cocaine and Amphetamines.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide (8e). Chapter 187
“Prison Medicine.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide (8e). Chapter 301
Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine, induced coronary vasoconstriction by beta adrenergic blockade. Ann Intern Med. 1990;112:897–90
Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94(6):608–610
Ibrahim M, Maselli DJ, Hasan R, Hamilton A. Safety of β-blockers in the acute management of cocaine-associated chest pain. The American Journal of Emergency Medicine. 31(3):613-616.
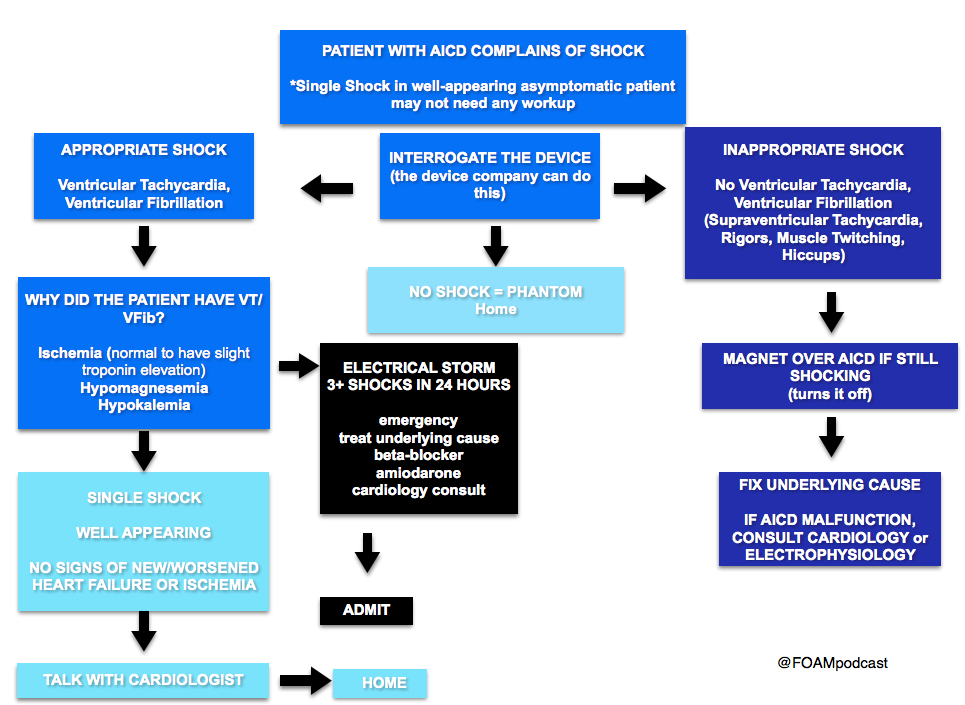
We delve into core content on implantable cardiac devices using Rosen’s (8th edition), Chapter 80 and Tintinalli (8th edition)
Generously Donated Rosh Review Questions
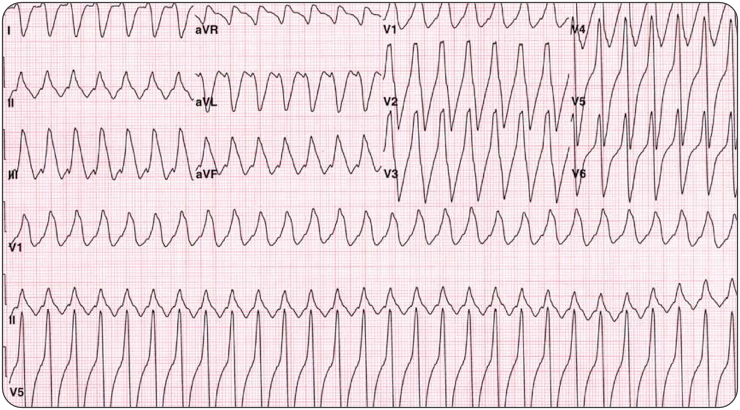
Question 1. A 44-year-old man with an automatic implantable cardioverter-defibrillator (AICD) in place presents with weakness and palpitations. Vitals are HR 180, BP 83/53, RR 28. His ECG is shown below. [polldaddy poll=9378494]
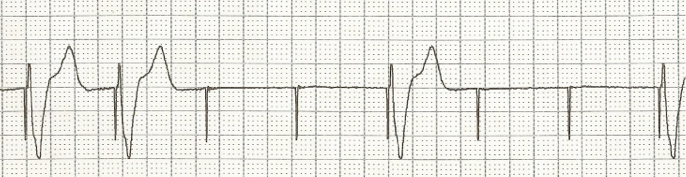
Question 2. A 76-year-old woman presents to the Emergency Department with generalized weakness and fatigue. She had a pacemaker placed one month ago. [polldaddy poll=9378495]
Answers
Electrical cardioversion. This patient presents with unstable ventricular tachycardia and should immediately be electrically cardioverted. AICDs are placed for a number of indications but the goal is the treatment of ventricular dysrhythmias, particularly ventricular tachycardia (VT) and ventricular fibrillation (VFib). All AICDs have a right ventricular lead that is used for sensing. During insertion, the cardiologist determines the parameters for the device to deliver a shock. Despite the presence of these devices, patients may still present in ventricular dysrhythmias that have not been shocked if the device is malfunctioning. Patients may also experience inappropriate shocks. Regardless of the presence of the device, if a patient presents in an unstable dysrhythmia,electrical cardioversion or defibrillation (depending on the circumstance) should still be performed. This patient presents with ventricular tachycardia and hypotension and device failure. It is recommended that if a shock is to be delivered in a patient with an AICD that the pads not be placed over the device site. Otherwise, the presence of a device is not a contraindication to external electrical cardioversion/defibrillation.
Amiodarone (A) and procainamide (D) are antidysrhythmic agents that can be used in the treatment of stable ventricular tachycardia. Placing a magnet over the AICD site (C) may be beneficial in treating patients who are receiving inappropriate shocks.
A. Failure to capture can range from complete absence of pacemaker activity to pacemaker spikes being seen but not resulting in depolarization of the myocardium. Complete absence of activity can be due to battery depletion, fracture of the pacemaker lead (which is uncommon with today’s technology) or disconnection of the lead from the generator. Intermittent failure to capture is commonly due to lead displacement and is most likely to happen within the first month of placement. Failure to pace can also be due to impaired endocardium, which despite an intact and normally functioning pacemaker, will not depolarize properly. Causes include ischemia or infarction, hyperkalemia or use of class III antiarrhythmic drugs. Overpacing (B) can occur when atrial flutter develops during dual chamber pacing. The pacemaker may sense the atrial flutter waves resulting in a rapidly paced ventricular rate. A “runaway pacemaker”, a pacemaker that causes extreme increases in pacing rates due to malfunction, is very unlikely with current pacemaker technology. In both of these cases, placing a magnet over the pacemaker will switch it from demand to fixed mode and may terminate the tachycardia. Oversensing (C) occurs when the pacemaker senses electrical activity that is not of cardiac origin and erroneously inhibits the generator. This may result in bradycardia. Undersensing (D) occurs when the pacemaker can not adequately sense the intrinsic electrical activity of the heart. If the pacemaker is in an inhibit mode, this can result in the pacemaker firing inappropriately.
References:
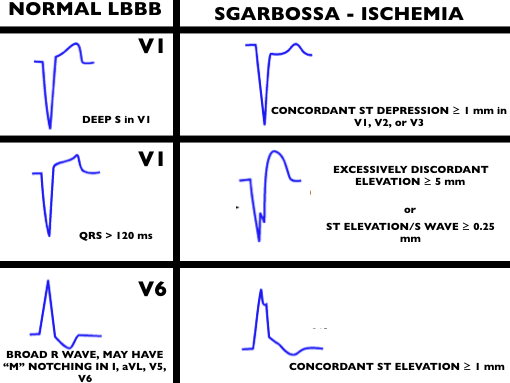
1. Sgarbossa EB, Pinski SL, Barbagelata et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. N Engl J Med. 1996 Feb 22;334(8):481
2. Smith SW, Dodd KW, Henry TD et al. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012 Dec;60(6):766-76.
3.Cai Q, Mehta N, Sgarbossa EB, Pinski SL, Wagner GS, Califf RM, Barbagelata A. The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: from falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time? Am Heart J. 2013 Sep;166(3):409-13. doi: 10.1016/j.ahj.2013.03.032.
Life in the Fast Lane Research and Reviews (LITFL R&R) #121 featured a section on the new American Gastroenterology Association (AGA) guidelines on diverticulitis. The game changer? Antibiotics aren’t a requirement in select patients with uncomplicated acute diverticulitis [1].
The guidelines based this recommendation on two studies, previously covered by Dr. Ryan Radecki on Emergency Medicine literature of note over the past 3 years. This post details a prospective observational study on antibiotics for acute diverticulitis [2]. In another post, Dr. Radecki discusses an RCT of antibiotics (ABX) vs IV fluids only.
623 patients with an episode with a short history and with clinical signs of diverticulitis, with fever (>38 Celsius) and inflammatory parameters, verified by computed tomography (CT), and without any sign of complications (fistula, perforation, abscess) or signs of sepsis
Randomized to IVF only or IVF + antibiotics
Primary Outcome – 6 patients (1.9%) developed complications in the no ABX arm vs 3 patients (1.0%) in the ABX arm (not statistically significant). Overall study complication rate was 1.4% [3].
Of note, since 2012, the Cochrane Review suggests that antibiotics may not be necessary in uncomplicated appendicitis [4].
A note on LITFL R&R – every week this blog post features 5-10 high yield articles, culled from contributors across the globe from all kinds of literature – pediatrics, critical care, emergency medicine, etc. It is difficult to keep up with the literature and some have estimated that the number needed to read (NNR) to of 20-200, depending on the journal [5]. Those looking for high yield articles may find their time well spent focused on this cherry picked selection of articles.
Core Content
We delve into core content on diverticula and clostridium difficile using Rosen’s Medicine (8e), Chapters 31, 173 and Tintinalli’s Emergency Medicine: A Comprehensive Study Guide(7e) Chapters 76, 85.
Diverticulosis
Diverticula are small herniations through the wall of the colon (small outpouchings). Often this is asymptomatic, identified incidentally on imaging or colonoscopy. Most common cause of lower gastrointestinal bleeding (LGIB) in adults in the U.S.
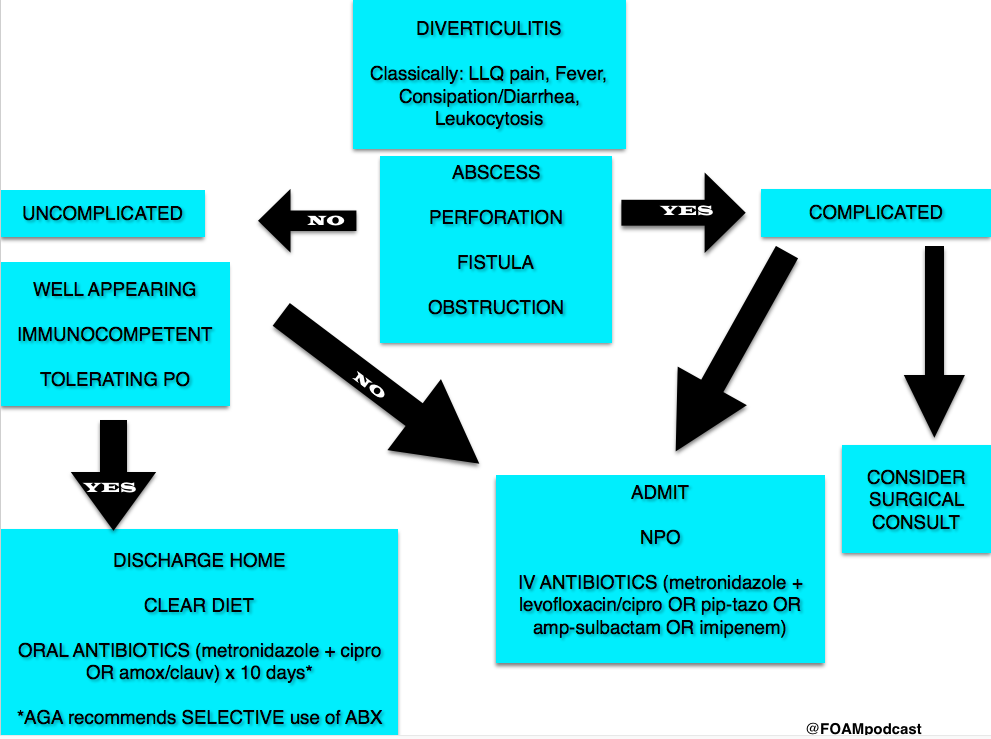
Diverticulitis
Diverticulitis Algorithm
Clostridium Difficile (c. diff)
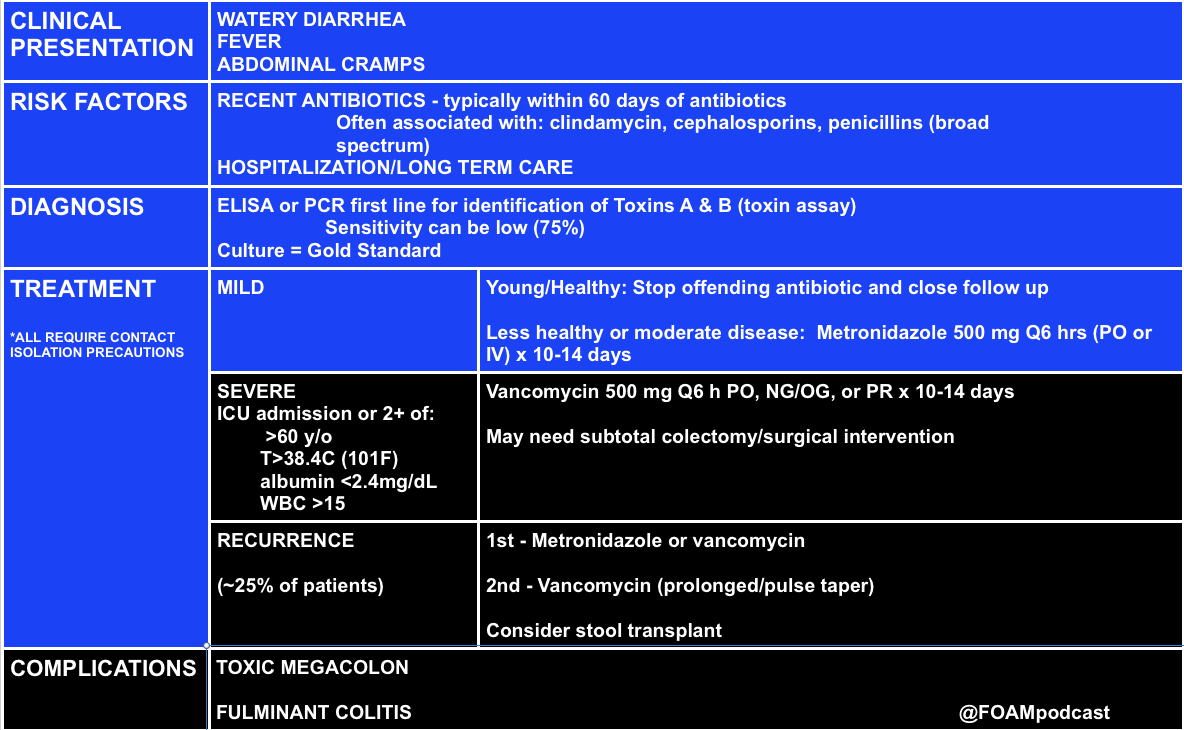
Note on testing – asymptomatic carriage rates of c.diff vary based on the population but may be between 3-50%. Textbooks quote a 3% carriage rate in newborns and rates of 20%-50% in hospitals and long term care facilities, respectively [10,11].
C. diff historically has a unique odor, refrains of “it smells like c. diff” echo in the halls. Yet this does not perform very well, essentially a coin flip based on a 2013 study by Rao and colleagues. They had 18 nurses smell 10 stool samples (5 c. diff positive and 5 c. diff neg) and found the median percent correct identification of c. diff positive vs negative was 45% [6].
Rosh Review Questions
Question 1. [polldaddy poll=9330955]
Question 2.A 75-year-old woman presents with several days of voluminous watery stools. She was discharged from the hospital one week ago following treatment for pneumonia. Stool studies reveal C. difficile toxin. [polldaddy poll=9333580]
Answers:
C. Patients who present with uncomplicated diverticulitis should be treated with oral antibiotics for 7-10 days. Diverticulitis is an inflammation of the diverticulum in the large intestine. In uncomplicated cases of diverticulitis, patients present with abdominal pain typically in the left lower quadrant with tenderness to palpation in the same area. Patients should not have peritoneal signs or masses on examination. Complicated diverticulitis is defined as the presence of either extensive inflammation or complications such as abscess, peritonitis or obstruction. Patients with uncomplicated diverticulitis can be empirically treated with antibiotics (typically as an outpatient) for 7-10 days. Patients with uncomplicated diverticulitis typically do not require CT imaging (A). Patients with complicated diverticulitis should be treated with intravenous antibiotics (B) and admitted to the hospital. Ultrasound (D) has shown promise in diagnosing diverticulitis but CT is the imaging modality of choice.
C.C. difficile infection is caused by a spore-forming obligate anaerobic bacillus that causes a spectrum of disease ranging from diarrhea to pseudomembranous colitis. C. difficile is the most common cause of infectious diarrhea in hospitalized patients in the United States. Risk factors for infection include broad-spectrum antibiotic use, particularly clindamycin, though other antibiotics have also been implicated. Additional risk factors include prolonged hospitalization, advanced age, and underlying comorbidities. The spectrum of clinical manifestations includes frequent watery stools to a more toxic clinical presentation with profuse stools (up to 20-30 per day), crampy abdominal pain, fever, leukocytosis, and hypovolemia. C. difficile colitis should be suspected in patients who develop diarrhea while taking or after recent cessation of antibiotics, or among recently discharged patients who develop diarrhea. Diagnosis is confirmed by identification of C.difficile toxin in the stool. Colonoscopy, while not usually necessary for diagnosis, reveals characteristic yellowish plaques in the intestinal lumen, confirming pseudomembranous colitis. Treatment for C. difficile infection depends on disease severity. Previously healthy patients with very mild symptoms may be managed by cessation of the offending antibiotic and close clinical monitoring. Oral metronidazole, 500 mg po every 6 hours for 10-14 days is the treatment for moderately severe colitis. Severely ill patients should be hospitalized and treated with oral vancomycin, 125 mg po every 6 hours for 10-14 days.
Isacson D, Thorisson A, Andreasson K, Nikberg M, Smedh K, Chabok A. Outpatient, non-antibiotic management in acute uncomplicated diverticulitis: a prospective study. Int J Colorectal Dis. 2015;30(9):1229–1234. doi:10.1007/s00384-015-2258-y.
Chabok A, Phlman L, Hjern F, Haapaniemi S, Smedh K. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br J Surg. 2012;99(4):532–539. doi:10.1002/bjs.8688.
Shabanzadeh DM1, Wille-Jørgensen P.Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev. 2012 Nov 14;11:CD009092. doi: 10.1002/14651858.CD009092.pub2.
McKibbon KA, Wilczynski NL, Haynes RB. What do evidence-based secondary journals tell us about the publication of clinically important articles in primary care journals? BMC Med. 2004;2:33.
Rao K, Berland D, Young C, Walk ST, Newton DW. The Nose Knows Not: Poor Predictive Value of Stool Sample Odor for Detection of Clostridium difficile. Clinical Infectious Diseases. 56(4):615-616. 2012.
“Chapter 85: Diverticulitis.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e.New York, NY: McGraw-Hill; 2011. p 578-581.
“Disorders of the Large Intestine.” Rosen’s Emergency Medicine, 8th e. p 1261-1275.
“Gastrointestinal Bleeding.” Rosen’s Emergency Medicine, 8th e. p 248-253.
“Infectious Diarrheal Disease and Dehydration.” Rosen’s Emergency Medicine, 8th ep 2188-2204.
“Chapter 76: Disorders Presenting Primarily with Diarrhea.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e.New York, NY: McGraw-Hill; 2011. p 534-535
We cover an EMcrit episode on Semantics of End of Life Discussions with Dr. Ashley Shreves as well as pearls from another favorite episode with her,Episode 93 – Critical Care Palliation. We can’t do these episodes justice summarizing them so listen to them. (Update: Apparently these podcasts were taken down due to personal reasons. From what we understand you may be able to obtain a copy by contacting the EMcrit site).
Screen who to have “the conversation” with looking for patients with signs of instability:
85 y/o and older
dementia/frailty
advanced cancer/disease
Key conversational points:
Lead with, ” I’m so worried about (the patient).”
“What do you think your (mom/dad/etc) would say about how she is now?”
“Got it.” Whether a family member agrees or disagree, let them know you heard them.
If a patient/family member are overly optimistic about the patient getting better one can try, “Many people find it helpful to talk about what would we should do if (the patient) doesn’t get better.”
Respect patient/family values that differ from yours. If the patient’s family just wants the heart beating regardless, and that’s ok. Per Dr. Shreves, this population is 5-10% and may be called “vitalists.”
Another key point Dr. Shreves emphasizes is that palliative care, comfort care, and allowing a natural death often mean escalating care – ensuring the patient is comfortable, clean, etc.
Core content
We delve into core content on vertigo using Rosen’s Medicine (8e) electronic chapter, “End of Life,”and Tintinalli’s Emergency Medicine: A Comprehensive Study Guide(7e) Chapter 297 “Death and Dying.”
DNAR (Do Not Attempt Resuscitation) – technically only speak to a patient’s wishes to receive CPR [3]. Problematic for several reasons, including:
Issue lies in the word “resuscitate,” which may be used to include fluids, antibiotics, vasopressors, advanced means of ventilation or, at the extreme, CPR. The AHA guidelines have moved to DNAR from DNR but even this language isn’t clear.
Major societies are moving towards the language AND, Allow Natural Death [4].
AND is preferred because it describes what happens and is more clear, is kinder language laden with reduced guilt
The TRIAD II-IV studies surveyed EMS personnel, physicians, and medical students respectively and provided the participants with an advance care directive as well as case scenarios. The participants then indicated whether a patient was a DNR or full code and the appropriate action. Both physicians and EMS providers performed poorly and variably, indicating that the directives were not clear [5-7].
Palliative care and hospice are not interchangeable. Palliative care has a more broad definition and
Palliative care: “An approach that improves quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual ” [1]. There is no time limit in this scenario.
Hospice care: subset of patients that a doctor has estimated likely has 6 months or less to live [1].
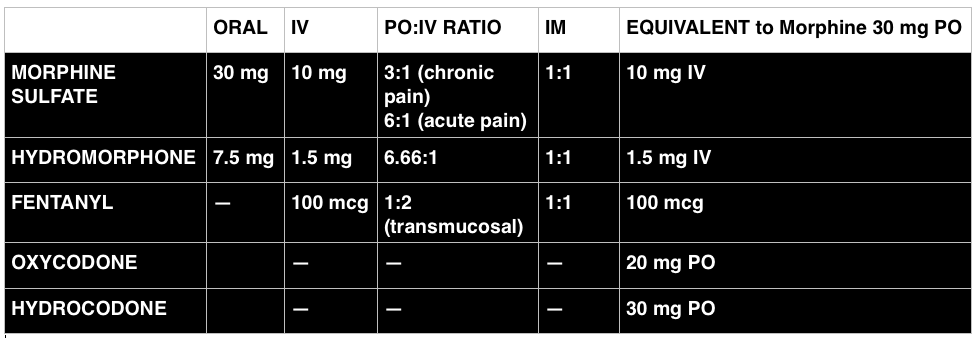
Opioid Equivalents
Many terminally ill patients or those at the end of their life are on chronic opioids. While the opioid epidemic is a problem, this is not the appropriate population from which we should withhold appropriate analgesia. It can be difficult to convert between dosages to adequately treat a patient’s pain. Here’s a free calculator.
References
Online Chapter. End of Life. In: Marx JA, Hockberger RS, Walls RM eds. Rosen’s Emergency Medicine, 8th e.
Chapter 297. Death and Dying. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds.Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011.
Breault JL. DNR, DNAR, or AND? Is Language Important? Ochsner J. 2011;11(4):302
Mirarchi FL, Kalantzis S, Hunter D, McCracken E, Kisiel T. TRIAD II: do living wills have an impact on pre-hospital lifesaving care? J Emerg Med. 2009;36(2):105–15. doi:10.1016/j.jemermed.2008.10.003.
Mirarchi FL, Costello E, Puller J, Cooney T, Kottkamp N. TRIAD III: nationwide assessment of living wills and do not resuscitate orders. J Emerg Med. 2012;42(5):511–20. doi:10.1016/j.jemermed.2011.07.015.
Sleep through 2015? We picked the minds of some brilliant Emergency Medicine folk and came up with this short list of important happenings.
TRAUMA
FAST (Focused Assessment using Sonography in Trauma) guided resuscitative – thoracotomy. (Recommended by Haney Mallemat, Rob Orman).
Bottom Line: If a trauma code comes in and has neither cardiac activity nor pericardial effusion on FAST, the odds of survival are essentially nil. Inaba and colleagues found the following:
Population: 187 patients at LA/USC deemed “appropriate” for thoracotomy (at this institution: penetrating trauma patients with absent vital signs and blunt trauma patients with a loss of vital signs en route or in the resuscitation bay).
Intervention: Emergency medicine resident performed FAST before/concurrent with thoracotomy
Outcome: Of the 126 patients without cardiac activity on FAST, none survived.
Many of the patients with cardiac activity did not survive, as well. This paper gives individuals guidance to make the decision to crack the chest but has stirred up a debate as to whether this would lessen educational opportunities for a potentially heroic procedure.
Say NO to long backboards (Recommended by Lauren Westafer). In January 2015, ACEP recommended against the use of long backboards. Many state and local protocols shifted away from moving this some time ago and even more since. The FOAM community has been up in arms about the inefficacies and harms of backboards for quite some time, again echoing that FOAM can serve as a forecaster for change to make it less cognitively distressing when time to change our practice.
RESUSCITATION
Peripheral Vasopressors (Recommended by Haney Mallemat, Rob Orman) – We detail the literature underlying the use of peripheral vasopressors in this podcast.
They think that the combination of a systematic review by Loubani et aland The Cardenas-Garcia study, peripheral vasopressors may be safely run through large bore peripheral IVs proximal to the antecubital fossa. Note: These should be closely monitored (protocolized is best) and short durations (<6 h) have been associated with minimal complicaitons.
SEPSIS
Intravenous fluids in sepsis (Recommended by Haney Mallemat). The PROMISE trial was published in early 2015, adding to ProCESS and ARISE. In these studies, patients typically got 2 L of crystalloid upfront and then 2L in the first 6 hours. Over 3 days after enrollment, most got just under 4 L. Most patients received under 6L IVF. There has been a movement for more judicious use of fluids in sepsis rather than dumping 4-6 L of IVF upfront. Marik articulately explained this in this article.
Mallemat challenges us: Before giving a fluid bolus use ultrasound and ask these questions, “Does the LV need it, and can the RV take it?”
CMS Core Measure (Recommended by Jeremy Faust). The National Quality Forum has been pushing for Measure 0500 See this EMcrit podcast on this topic.
Sexual intercourse 3-4 times per week may aid in expulsion of distal kidney stones. This year, two large studies by Pickard et al and Furyk et al demonstrated no benefit in stone passage for ureterolithiasis (particularly in stones <5 mm). Then, a paper by Dolouglu et al excited many folks, if for entertainment value. Since tamsulosin doesn’t seem to help, what about sexual intercourse, 3-4 times per week, in male patients with partners?
In this study the mean expulsion time did not differ significantly between groups.
MEDICAL EDUCATION
Merging of FOAM resources. (Recommended by Michelle Lin). Blogs and podcasts are growing and often supplement one another. Dr. Lin predicts the future will be in these conglomerates (ex: merging of EMcrit and PulmCrit and massive undertakings such as ALiEM and CandiEM).
Merging of FOAM with traditional journals. (Recommended by Michelle Lin). Projects such as the Skeptic’s Guide to Emergency Medicine have merged with Academic Emergency Medicine and the Canadian Journal of Emergency Medicine (ex: SGEM HOP, journal paper) and massive FOAM resource ALiEM has also collaborated with Annals of Emergency Medicine (Ex:Journal club, paper). The merging of FOAM with paid, traditional resources is the future, per Dr. Lin.
OVERDIAGNOSIS
Overdiagnosis is a problem, and people are starting to rage against it. (Recommended by Lauren Westafer). An Overdiagnosis conference exists and JAMA Internal Medicine has a series of articles, “Less is More,” frequently detailing evidence of overdiagnosis.
One of 2015’s prominent articles for emergency physicians was the Hutchinson et al study. In this study, CTPA scans read as positive for pulmonary embolism underwent review by 3 chest radiologist who adjudicated that, actually, 25.9% of the “positive” scans (n=45) did not actually have pulmonary embolisms. The harms from this exist beyond the risk of anticoagulation (think about how an ED approach for a myriad of complaints differs for a patient with a history of thromboembolism).
The FOAM community swelled with appreciation and respect for the late Dr. John Hinds. Please watch his SMACC talk, “Crack the Chest, Get Crucified,” in which his excellence in medical education shines, delivering pearls for nearly anyone.
Better pain control for uncomfortable patients. Many patients with hip and femoral neck fractures are elderly. As such, opioids may be underdosed or pain medications may be used sparingly in these patients. Further, patients may still have pain with transfers.
Reduction in opioids. Opioids relieve pain but often have deleterious side effects. In addition to hypotension and allergic reactions, opioids may cause delirium.
Why don’t we do it? As a knowledge translation project, Dr. Milne’s podcast aims to propagate the best available, clinically relevant information to practitioners to mitigate the knowledge translation gap as much of the other world provides these blocks routinely to suspected fractures. A study by Haslam and colleagues from Canada suggests that while emergency providers know regional anesthesia is good in this scenario there are other barriers to adoption in North America [2]. Systemic barriers exist and include consultant worries about compartment syndrome, which is largely unfounded [3]. See this post for a more in-depth exploration.
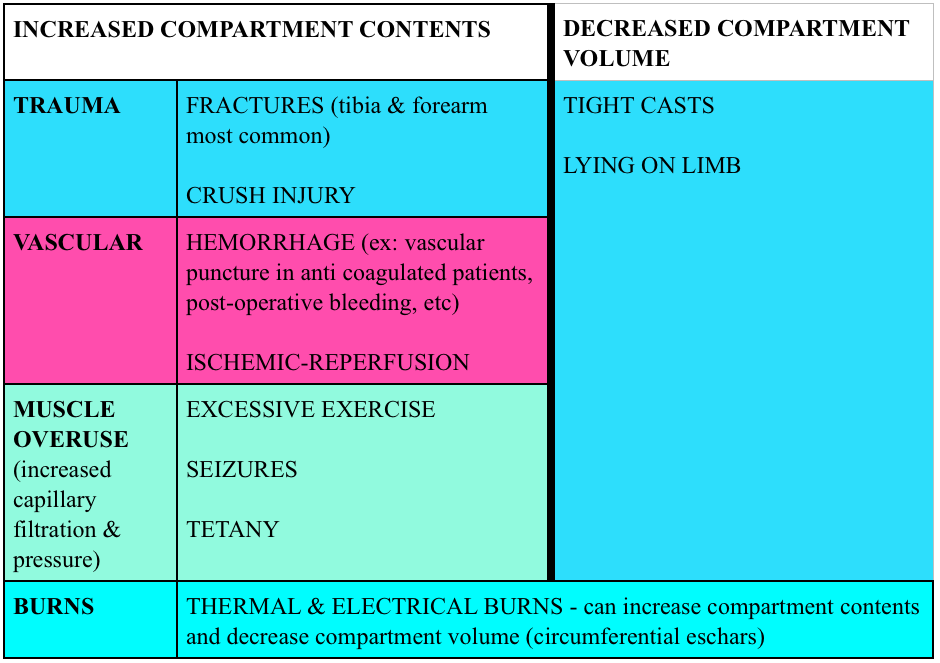
Compartment syndrome is typically caused by too much pressure in a confined space. Compartments are often surrounded by fascia and tissue with limited ability to stretch. When the volume in the compartment increases or external forces compresses the compartment, blood flow in and out of the compartment are compromised. Certain areas of the body are more predisposed to compartment syndrome (classics are the lower leg in tibia fractures and the forearm compartments).
Causes: Most cases of compartment syndrome are caused by fractures (~75%) but certainly not all.
Diagnosis:
Clinical. Classically this was taught as the 5 P’s (pain, parethesias, pallor, pulselessness, poikilothermia). Yet, many of these perform poorly in real life.
Compartment pressures. Many commercial devices exist to measure compartment pressures, yet these readings have poor specificity for compartment syndrome.
Historically, compartment pressures >30 mmHg or a delta pressure (Diastolic pressure minus the compartment pressure) <20-30 mmHg has indicated compartment syndrome.
Studies have measured compartment pressures on long bone fracture patients NOT suspected of having compartment syndrome and found that acting based on pressures would have resulted in 24-35% overdiagnosis (depending on a delta pressure cut-off of 20 mmHg and 30 mmHg respectively) [4-5]
Treatment:
Fasciotomy. Suspect compartment syndrome? Call surgery. In the the meantime, remove constrictive bands or clothing, give analgesia, place the limb in a dependent position, assess for rhabdomyolysis.
1. A 24-year-old long distance athlete was brought to the emergency room complaining of severe leg pain in his left anterior lower leg. The pain became worse while running his ultra marathon yesterday and subsided after he finished. However he went for a run today and the pain returned. He describes the pain as a burning, tight pain that is 10/10. On physical exam he is in exquisite discomfort. There are no signs of trauma or broken bones. The pain is worsened on passive stretching of the leg. On palpation of his legs there is a firm wooden feeling. Distal pulses are palpated however his left leg does appear very pale. He has diminished 2-point sensory discrimination in his left leg compared to his right leg. [polldaddy poll=9241018]
2. You obtain a radiograph of a patient who was in a MVC. His GCS is 15. While being observed in the ED, the patient requests increasing doses of pain medication and is complaining of a deep, burning, unrelenting pain to his left lower extremity. He also states that he now feels tingling in his calf. [polldaddy poll=9241033]
Answers.
Compartment syndrome is a serious emergency complication that should be considered whenever pain and paresthesias occur in an extremity after a fracture within an enclosed osseofascial space. It is caused by increased pressure within the compartment space that prevents adequatetissue perfusion. Compartment syndrome is most commonly associated with closed long-bone fractures of the tibia, but it can occur with isolated soft tissue trauma and even in open fractures. It has been described in a variety of situations such as prolonged procedures in the lithotomy position, the tuck position (knees tucked to chest for lumbar surgery), bedridden patients, from a spontaneous hemorrhage, and even the application of excessive traction in the reduction of a fracture. Compression dressings (A) and external wrappings should be avoided; increased compression will worsen perfusion. Elevating the limb (B) results in reduction in the local arteriovenous gradient and may be counterproductive and exacerbate compartment syndrome. It is best to keep the extremity level or slightly elevated (<10 degrees). Pressures <30 mmg Hg (C) generally do not produce compartment syndrome. The best measure of adequate limb perfusion, however, is not absolute compartment pressure but rather the differential between diastolic blood pressure and absolute compartment pressure. A pressure differential <30 mm Hg is considered by most to be an indication for emergent fasciotomy. However, with strong clinical suspicion, a fasciotomy may be required at any pressure differential as this is largely a clinical diagnosis. The initial presentation of compartment syndrome (E) usually begins with pain with passive stretching of the muscle groups, paresthesias with decreased sensation, and pain that is out of proportion to exam. Pallor and the loss of pulses are late and ominous findings.
Compartment syndrome is a serious emergency complication that should be considered whenever pain and paresthesias occur in an extremity after a fracture within an enclosed osseofascial space. It is caused by increased pressure within the compartment space that prevents adequate tissue perfusion. Compartment syndrome is most commonly associated with closed long-bone fractures of the tibia, but it can occur with isolated soft tissue trauma and even in open fractures. It has been described in a variety of situations such as prolonged procedures in the lithotomy position, the tuck position (knees tucked to chest for lumbar surgery), bedridden patients, from a spontaneous hemorrhage, and even the application of excessive traction in the reduction of a fracture. Compression dressings (A) and external wrappings should be avoided; increased compression will worsen perfusion. Elevating the limb (B) results in reduction in the local arteriovenous gradient and may be counterproductive and exacerbate compartment syndrome. It is best to keep the extremity level or slightly elevated (<10 degrees). Pressures <30 mmg Hg (C) generally do not produce compartment syndrome. The best measure of adequate limb perfusion, however, is not absolute compartment pressure but rather the differential between diastolic blood pressure and absolute compartment pressure. A pressure differential <30 mm Hg is considered by most to be an indication for emergent fasciotomy. However, with strong clinical suspicion, a fasciotomy may be required at any pressure differential as this is largely a clinical diagnosis. The initial presentation of compartment syndrome (E) usually begins with pain with passive stretching of the muscle groups, paresthesias with decreased sensation, and pain that is out of proportion to exam. Pallor and the loss of pulses are late and ominous findings.
References:
“Hip and Femur Injuries.” Chapter 270. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide.
We cover a trick of the trade from Dr. Brian Lin, posted on the Academic Life in Emergency Medicine (ALiEM site) on hemostasis in finger tip avulsions. Dr. Lin also has his own excellent FOAM site on all things laceration – LacerationRepair.com.
No clear “golden period” for laceration repair [4-6]. Rosen’s and Tintinalli recommend using clinical judgment as a guide.
Risks for Infection:
Diabetes
Length of laceration (>5 cm)
Location of the wound
Degree of contamination [6]
Age of wound when approximated (i.e. “golden period”) has not been found to be an independent risk factor). Rosen’s sites use of epinephrine as a risk but only cites a paper by Barker et al from 1982 in which tetracaine/epinephrine/cocaine was applied to wounds inflicted by researchers that were inoculated by s. aureus.
Question 1.An 18-year-old woman presents with a laceration to her face from a dog bite that occurred 24 hours ago. The patient owns the dog. Examination reveals a 4 cm laceration to the left cheek with no signs of infection. [polldaddy poll=9180209]
Question 2. A 30-year-old man presents with a 2 cm linear laceration through his right eyebrow that he sustained after hitting his head on the kitchen cabinet. You determine that the wound will require repair with sutures. [polldaddy poll=9180210]
Answers
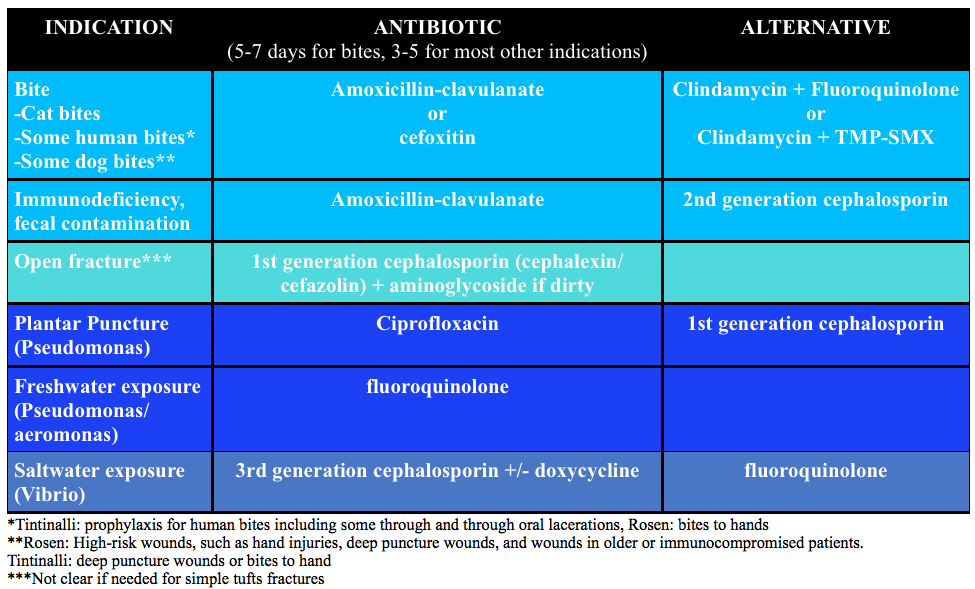
Mammal bites to any part of the body should be copiously irrigated and explored followed by an assessment for primary closure. In this patient, primary closure is recommended as the laceration is on the face. Canine bites often involve laceration as well as crush injury to tissue depending on the size of dog. The presence of a crush injury may make primary wound repair difficult. Additionally, devascularization of the tissue may make primary closure contraindicated as the risk of infection increases. Classically, it was taught that lacerations sustained from dog bites should be irrigated, given antibiotics and not primarily repaired because of these risks. However, more recent literature has shown that the risk of infection was no different for primary closure versus healing by secondary intention. Additionally, if the laceration is to a cosmetic area like the face, primary repair should be attempted. As with any laceration, tetanus status should be updated. Copious irrigation and wound exploration is central to good wound care. Exploration should pay particular attention to the presence of foreign bodies especially teeth, which may break off during the bite. Antibiotics (A & C) are not routinely needed for dog bites despite classic teaching. Antibiotics should be reserved for patients with signs of infection, multiple comorbidities or large wounds with gross contamination. If antibiotics are given, they should primarily cover Staphylococcus and Streptococcus species, as these are the predominant organisms in the canine oral cavity. Eikenella and Pasturella are less commonly responsible for infections. Irrigation and antibiotics alone (A) would be indicated for dog bites that are grossly infected or have large defects that cannot be primarily closed. Wound closure and antibiotics without irrigation (D) is also contraindicated as copious irrigation is central to proper wound management.
A pair of clean, non-sterile gloves can be worn by the physician (and any assistants) during laceration repair. The use of sterile gloves has not been proven to be associated with lower infection rates and is not required. Wounds must be prepped prior to closure. This generally involves cleaning and draping the wound, providing local or regional anesthesia, copious irrigation and exploring the wound to evaluate the integrity underlying structures and identify any foreign bodies. The skin surrounding a wound should be cleansed with either 10% povidone-iodine (C) or chlorhexidine gluconate solution. In general, these commercially available antiseptics should not be used for wound irrigation, as they can be toxic to the tissues. Irrigation should then follow with copious amounts of tap water or saline (at least 250 mL). This is best achieved with a large volume syringe attached to an 18-gauge needle or another commercially available irrigation device that achieves adequate pressure for irrigation. Alternatively, patients can irrigate at the sink if the laceration is in area that allows for this. Shaving of hair been shown to increase the risk of infection and should generally be avoided. It is best to apply a small amount of petroleum- or water-based lubricant to the hair to keep it out of the wound. Alternatively, hair can be clipped with scissors when necessary. Eyebrows (B) in particular should not be shaved as they provide anatomic landmarks that aid in wound approximation and removal results in poor short- and long-term cosmetic effect. In general, non-complex facial wounds are closed with nonabsorbable suture material, such as nylon or polypropylene. Most commonly this will be done with 6-0 suture, as it provides the best cosmetic effect. The use of 3-0 (D) and 4-0 suture is reserved for repair of fascia or wounds that are under high stress, such as those that overly major joints or involve the scalp.
American College of Emergency Physicians: Clinical policy for the initial approach to patients presenting with penetrating extremity trauma. Annals of emergency medicine. 33(5):612-36. 1999. [pubmed] **A past policy, no current clinical policy
FOAMcast brings you pearls from conferences we attend and presently it’s the American College of Emergency Physicians annual meeting, ACEP15 in Boston.
On this episode we cover the following topics:
Foodborne Illnesses – Dr. David Pigott
Wound Management – Dr. Benjamin Lawner
Irrigation – Need 50-100 cc per centimeter of wound. To get adequate PSI, take an 18g angiocath on a 30 cc syringe = 4-15 PSI
Some predictors of poor healing and infection
Location – head and neck more vascular so less likely to get infected
Length – >5 cm more likely to have problems
Diabetics – microvascular damange makes healing more problematic
Tips for Presentations – Dr. Haney Mallemat (@CriticalCareNow)
Avoid bullet points
Be brief
Use a sans serif font (and only one font throughout)
FOAMcast brings you pearls from conferences we attend and presently it’s the American College of Emergency Physicians annual meeting, ACEP15 in Boston. On this episode we cover the following topics:
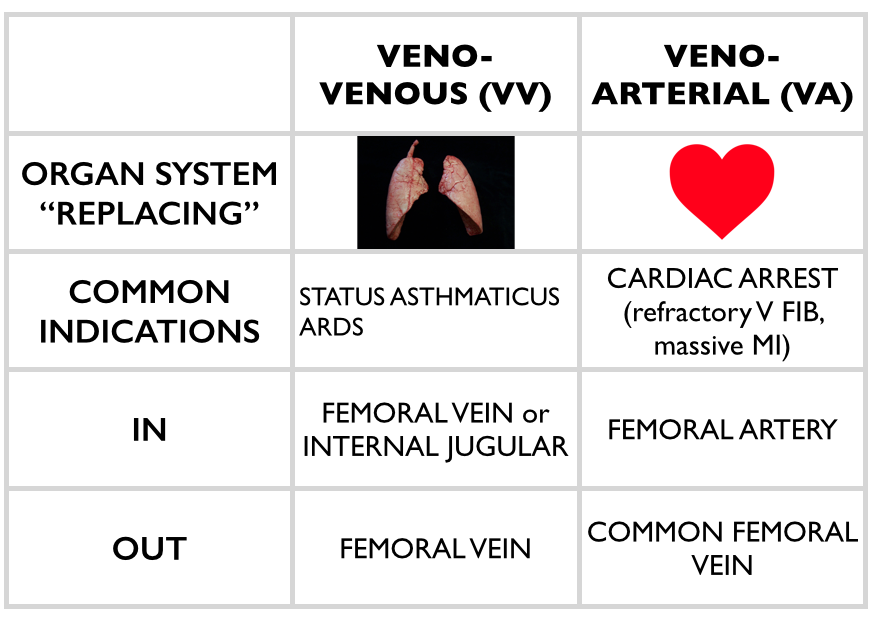
Extracorporeal Membrane Oxygenation (ECMO) – Dr. Haney Mallemat (@CriticalCareNow)
ECMO is promising in certain devestating disease processes – essentially heart or lung failure. For example, in the CHEER trial, the investigators had a 54% rate of neuro-intact survival after cardiac arrest with ECMO []. Yet, ECMO can be confusing. Dr. Mallemat simplified this for the emergency physician (see this site for more complete explanations)
Stop the Madness: Diagnostic Imaging in Nephrolithiasis – Workshop with Drs. Eddy Lang, Rebecca Smith-Bindman, Grant Innes, and Lauren Westafer