We are in Berlin for #dasSMACC and have lots of pearls to share from the speakers at this amazing conference. Talks will be released for free on the SMACC podcast over the next year, but this podcast holds some pearls that we thought couldn’t wait.
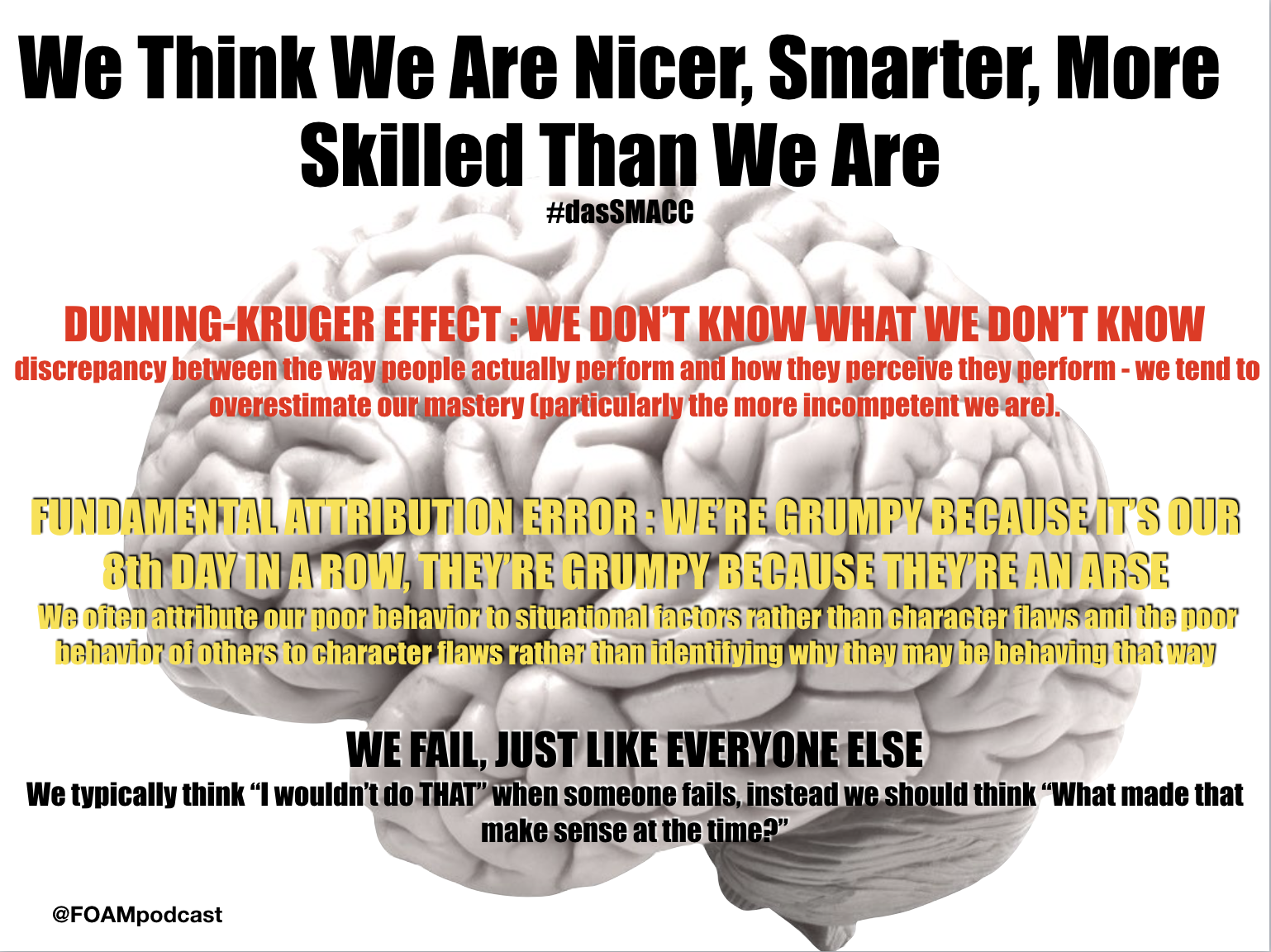
Overall trope of the conference….
for more on the Dunning-Kruger effect check out this post
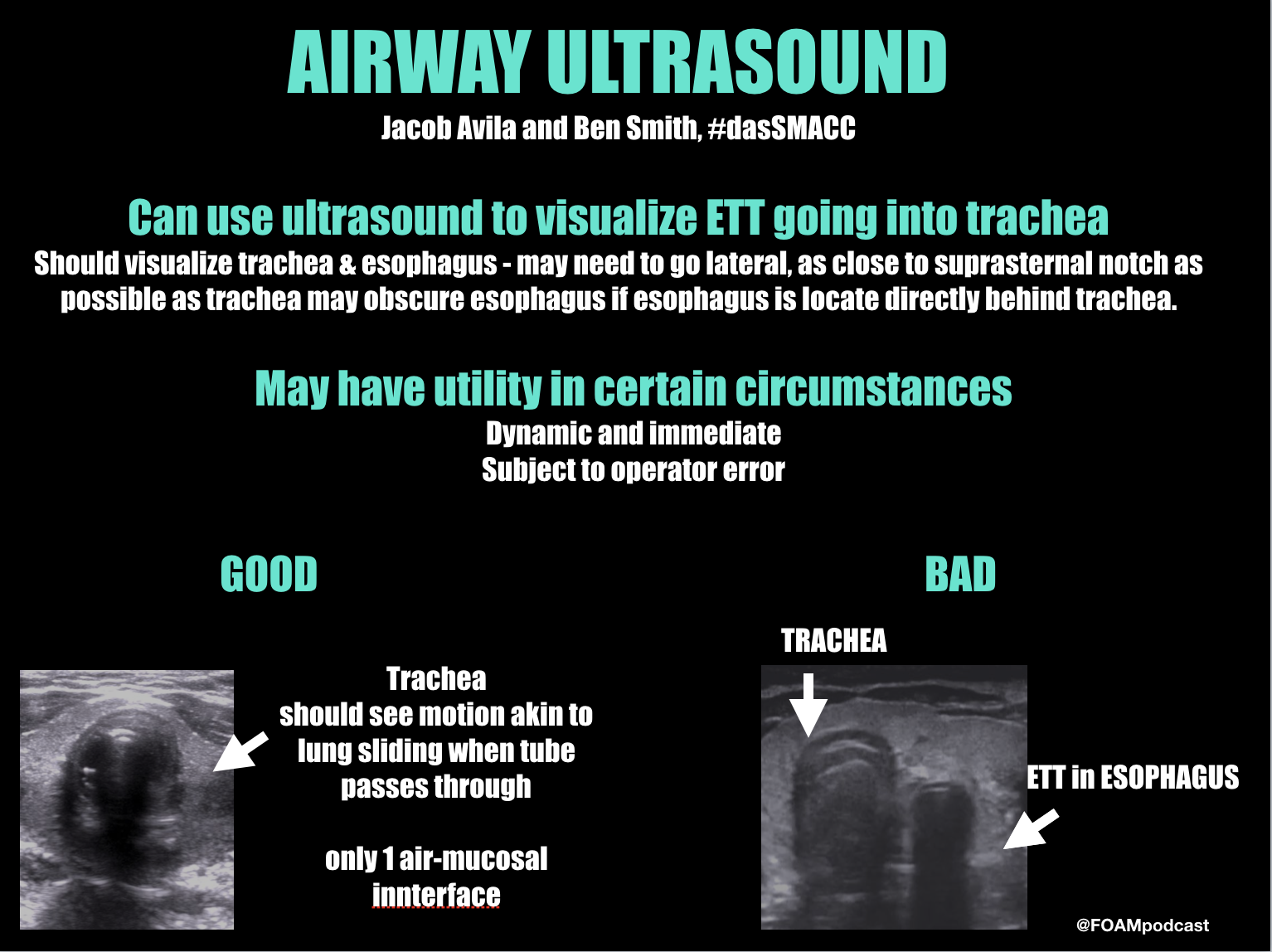
Drs. Jacob Avila and Ben Smith on Airway Ultrasound
Check out this 7-minute video on ETT placement confirmation using ultrasound
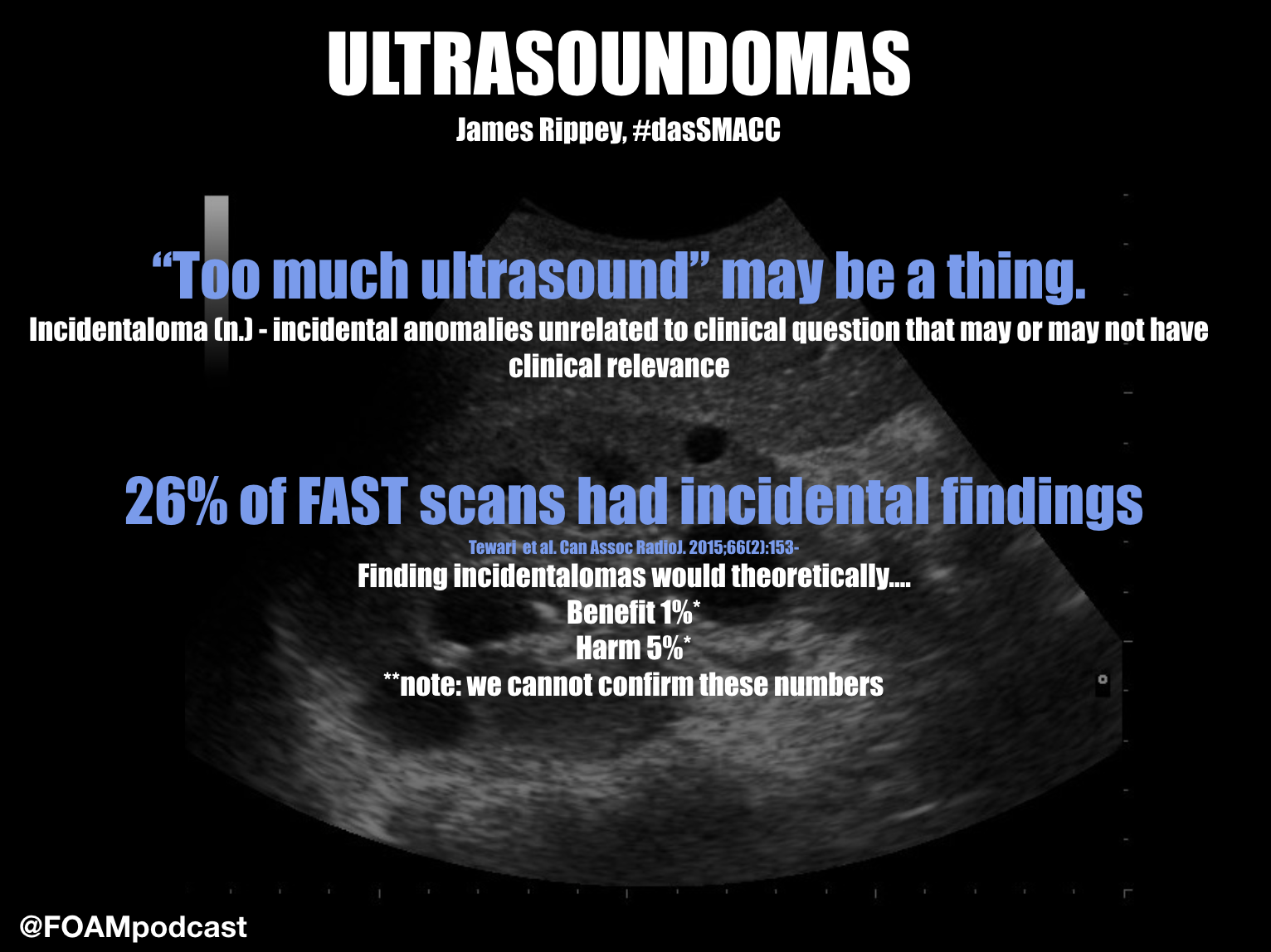
Dr. James Rippey on Point of Care Ultrasound Incidental Findings
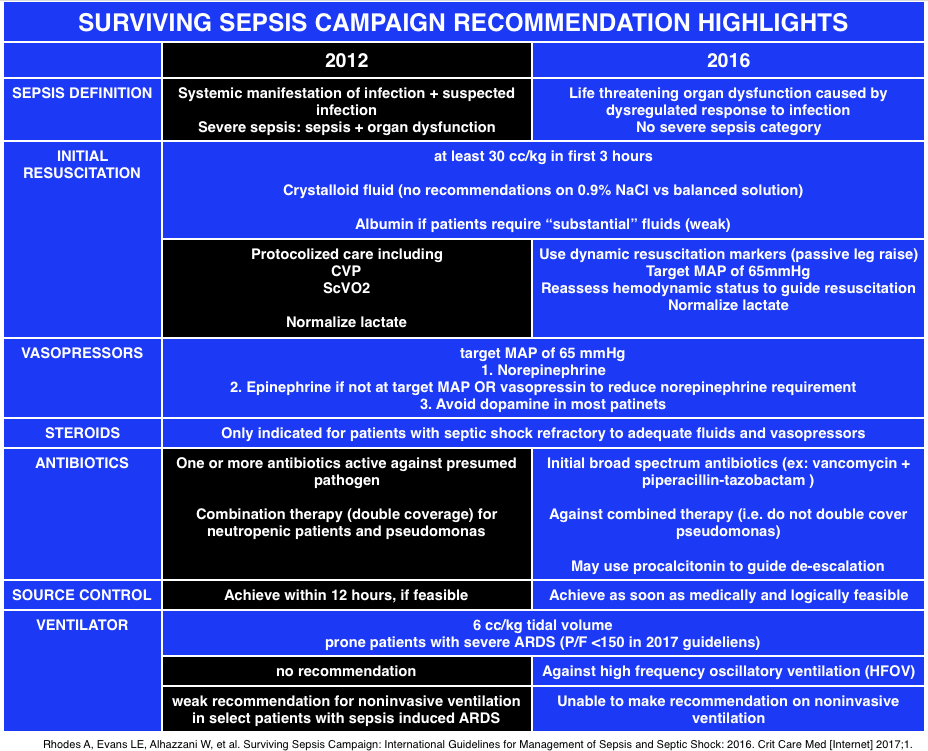
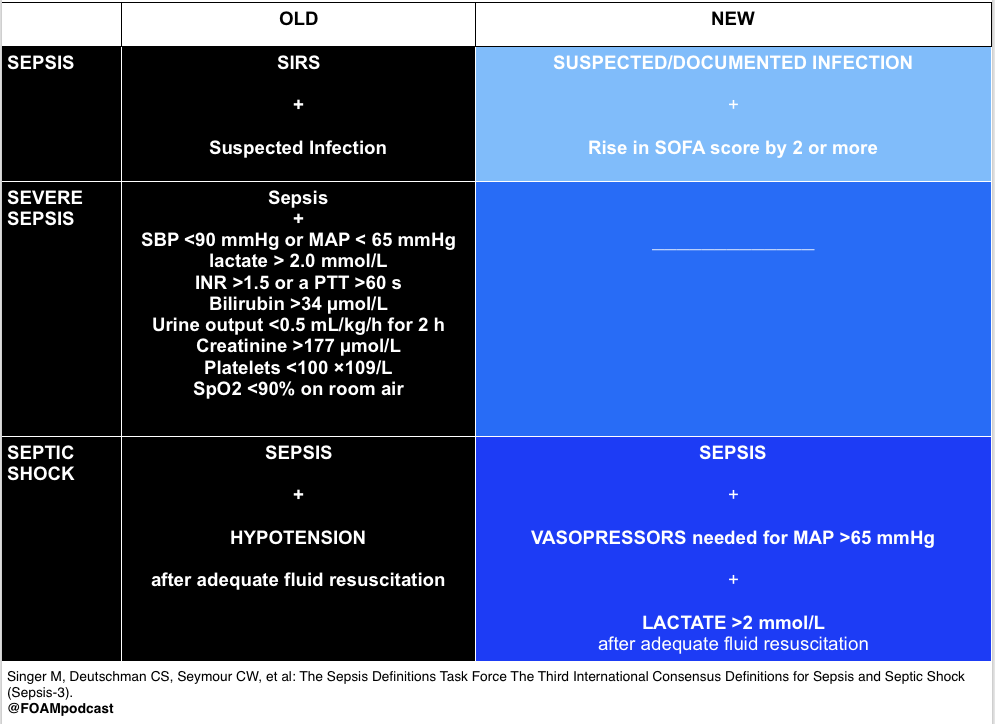
The new Surviving Sepsis Campaign Guidelines are out in Critical Care Medicine. The biggest change is the change in the definition of sepsis, which now uses the language of Sepsis 3.0, introduced in 2016. Other significant changes include dropping protocolized care (ex: early goal directed therapy), and recommending against combination antibiotic therapy (double coverage) for a single pathogen [1,2].
Bonus discussion on new validation study of qSOFA
References:
Opal SM, Rubenfeld GD, Poll T Van Der, Vincent J, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). 2016;315(8):801–10.
Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit Care Med [Internet] 2017;1.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of Clinical Criteria for Sepsis. Jama [Internet] 2016;315(8):762.
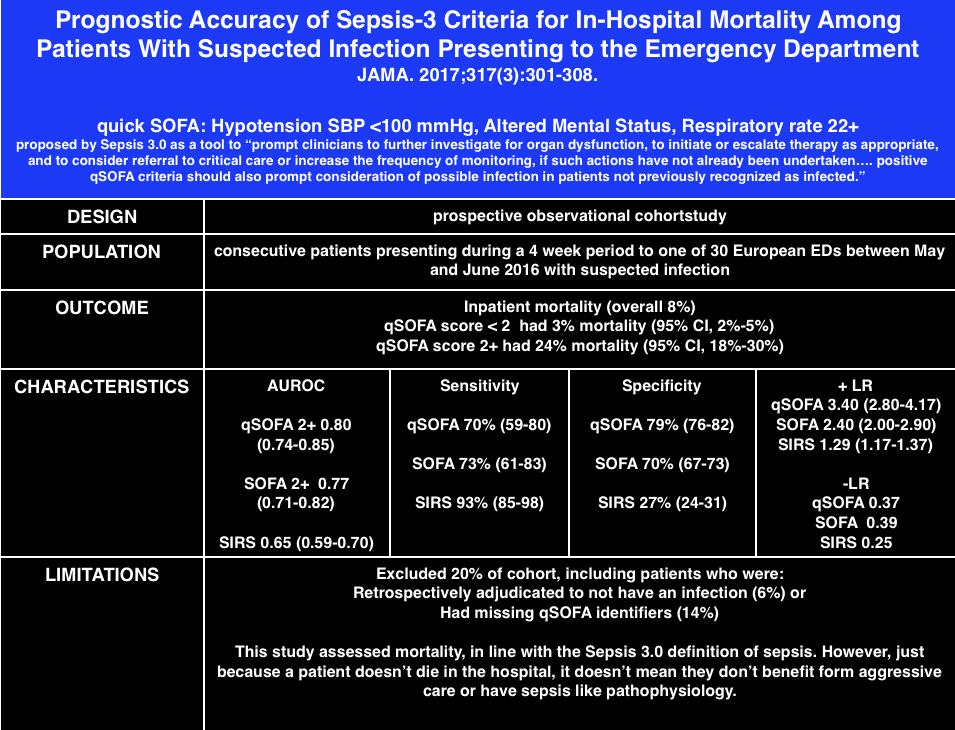
Freund Y, LeMachatti N, Krastinova E.Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients W.ith Suspected Infection Presenting to the Emergency Department. JAMA. 2017;317(3):267-268.
This iteration of sepsis discarded systemic inflammatory response syndrome (SIRS), noting it’s poor discriminatory ability. Further, these authors sought to define sepsis as a dysregulated response to infection, not just a normal response to infection (i.e. fever and tachycardia are normal responses to infection and therefore are, alone, not evidence of sepsis).
The quick SOFA score (qSOFA) also came out in hopes it “provides simple bedside criteria to identify adult patients with suspected infection who are likely to have poor outcomes.” It is not part of the sepsis definition but may help in identifying those that will die or have a 3 day ICU stay. Studies looking at the performance of qSOFA applied retrospectively to data sets have not been promising [1,2].
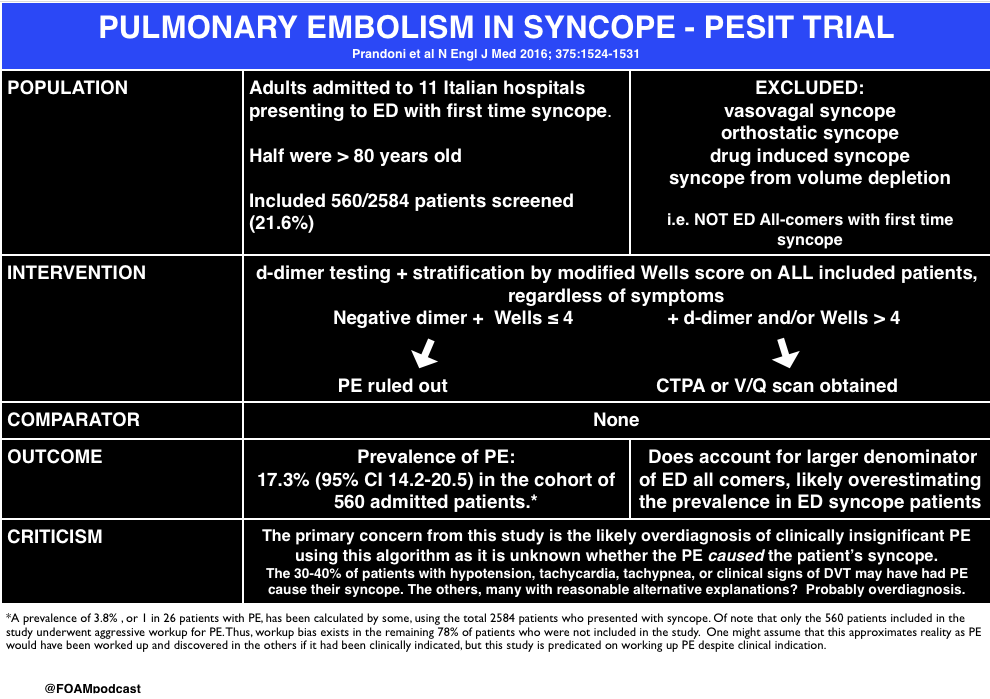
Prandoni et al. Prevalence of Pulmonary Embolism among Patients Hospitalized for Syncope. N Engl J Med 2016; 375:1524-1531. This trial is probably one of the most over-reacted to trials of 2016. News outlets, both by lay media and for health professionals overstated the claims of this trial.
Churpek MM, Snyder A, Han X et al. qSOFA, SIRS, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients Outside the ICU. Am J Respir Crit Care Med. 2016. [article]
Brabrand M, Havshøj U, Graham CA. Validation of the qSOFA score for identification of septic patients: A retrospective study. European Journal of Internal Medicine. 36:e35-e36. 2016. [article]
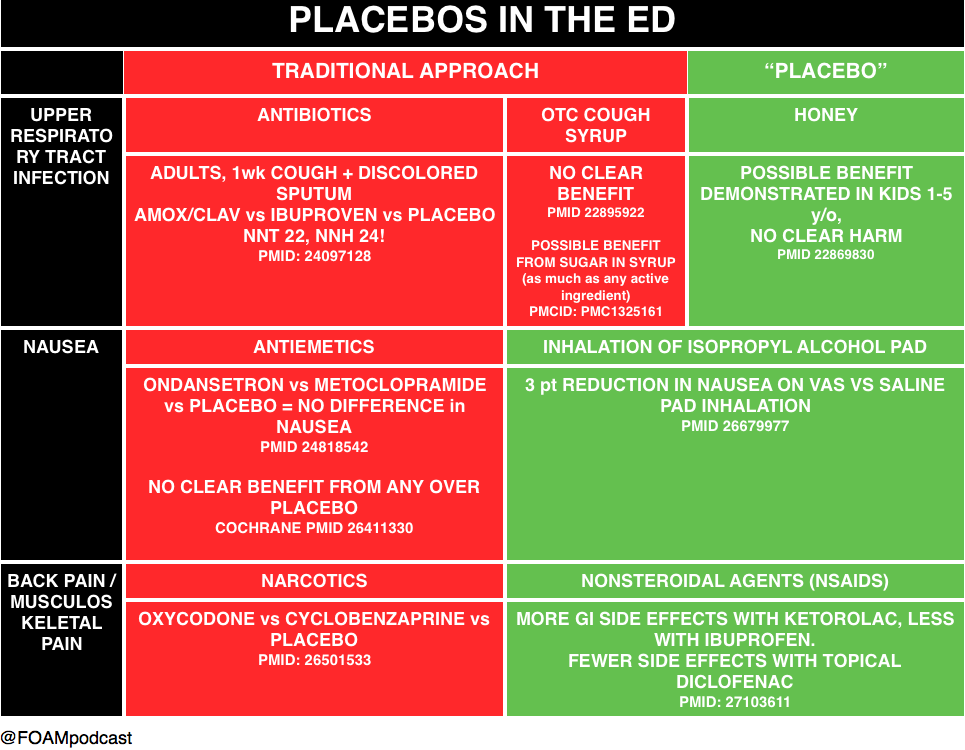
Llor C, Moragas A, Bayona C. Efficacy of anti-inflammatory or antibiotic treatment in patients with non-complicated acute bronchitis and discoloured sputum: randomised placebo controlled trial. BMJ (Clinical research ed.). 347:f5762. 2013. [pubmed]
Smith et al. Over-the-counter (OTC) medications for acute cough in children and adults in ambulatory settings. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD001831. DOI: 10.1002/14651858.CD001831.pub4.22895922
Dobson R. Cough medicines’ effect is mainly placebo. BMJ. 2006 Jan 7; 332(7532): 8. PMCID: PMC1325161
Cohen et al. Effect of Honey on Nocturnal Cough and Sleep Quality: A Double-blind, Randomized, Placebo-Controlled Study Pediatrics; originally published online August 6, 2012; PMID:22869830
Egerton-Warburton D, Meek R, Mee MJ, Braitberg G. Antiemetic use for nausea and vomiting in adult emergency department patients: randomized controlled trial comparing ondansetron, metoclopramide, and placebo. Annals of emergency medicine. 64(5):526-532.e1. 2014. [pubmed]
Furyk JS, Meek RA, Egerton-Warburton D. Drugs for the treatment of nausea and vomiting in adults in the emergency department setting. The Cochrane database of systematic reviews. 2015. [pubmed]
Beadle KL, Helbling AR, Love SL, April MD, Hunter CJ. Isopropyl Alcohol Nasal Inhalation for Nausea in the Emergency Department: A Randomized Controlled Trial. Annals of emergency medicine. 68(1):1-9.e1. 2016. [pubmed]
Friedman BW, Dym AA, Davitt M. Naproxen With Cyclobenzaprine, Oxycodone/Acetaminophen, or Placebo for Treating Acute Low Back Pain: A Randomized Clinical Trial. JAMA. 314(15):1572-80. 2015. [pubmed]
Derry S, Conaghan P, Da Silva JA, Wiffen PJ, Moore RA. Topical NSAIDs for chronic musculoskeletal pain in adults. The Cochrane database of systematic reviews. 4:CD007400. 2016. [pubmed]
We are in Las Vegas at ACEP 2016 and discuss high yield or cutting edge lectures each day.
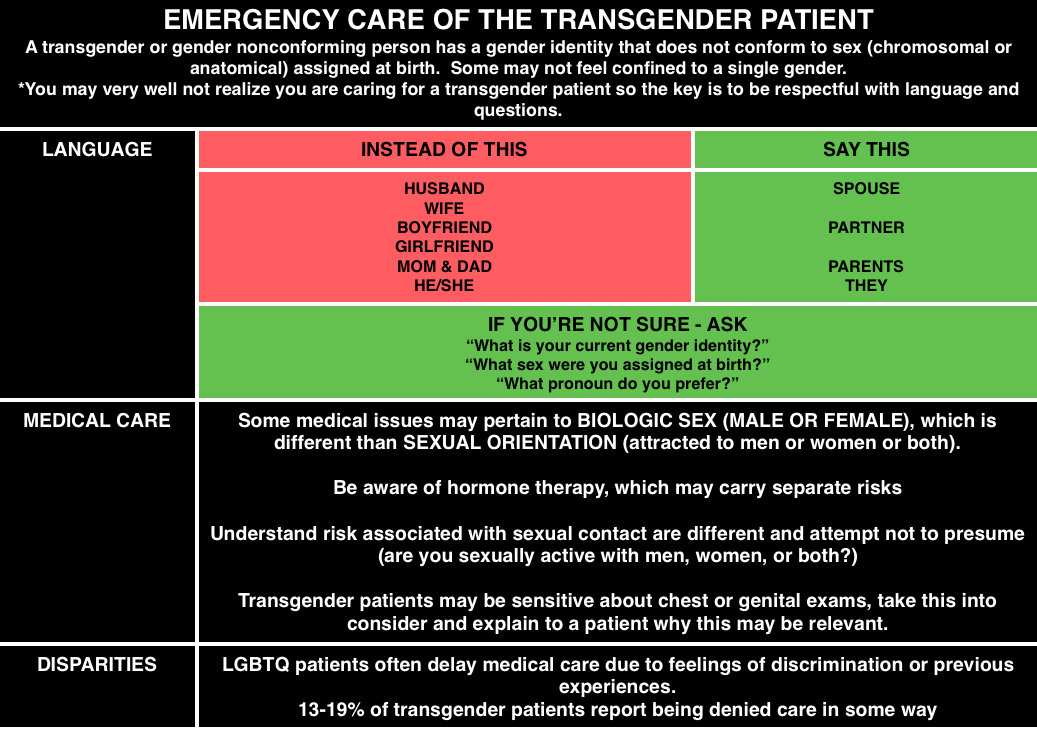
Dr. Anne Daul – Emergency Care of the Transgender Patient
Most emergency medicine physicians and trainees lack training in caring for LGBTQ patients, let alone transgender patients [1]. Many members of the LGBTQ community may have delays in medical care including 21% of transgender patients in a Canadian survey[2]. Also, according to a 2010 task force, 19% of transgender patients report being denied care in some way [3].
@FOAMpodcast
Here is a video from SMACC Dublin from Thom O’Neill on caring for LGBT youth
Check out these FOAM resources from EPMonthly and Mayo.
Dr. David Callaway – Active Shooter
2% of active shooter events take place in the health care setting.
Plan of Action in Active Shooter Scenario: AVOID DENY DEFEND TREAT
Avoid – stay away from the shooter.
Deny – deny them access to you or the area. Lock doors, block pathways, turn off the lights, make it more difficult for them.
Defend -.if necessary, defend yourself.
Treat – once you are safe, and the scene is safe, treat and care for your patients.
Dr. Kevin Klaur – Lawsuits
Documentation and discharge instructions repeatedly come up in lawsuits.
Documentation: If you document after the fact, particularly if there was a bad outcome – be straightforward that you are documenting after the fact. Do not document as though you do now know the outcome
Discharge – lawsuits often come up because discharge instructions or documentation were not sufficient. Klauer argues that it is not sufficient to state “patient improved, discharged home.” He urges us to document a repeat exam or show HOW they are improved.
Dr. Klauer also gave some general pearls on lawsuits – high numbers for orthopedics/missed fractures and administration of RhoGham. An additional pearl he gave was for cauda equina.
These patients often have small post void residuals because it’s a neurogenic problem, not a mechanical obstruction. Thus, if a patient has other features and has a post void residual of 100 cc, it’s not necessarily not cauda equina.
One ACEP16 lecturer talked about magnesium use in alcohol withdrawal – probably not ready for prime time, Cochrane agrees [4].
References:
Moll J, Krieger P, Moreno-Walton L. The prevalence of lesbian, gay, bisexual, and transgender health education and training in emergency medicine residency programs: what do we know? Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 21(5):608-11. 2014. [pubmed]
Bauer GR, Scheim AI, Deutsch MB, Massarella C. Reported emergency department avoidance, use, and experiences of transgender persons in Ontario, Canada: results from a respondent-driven sampling survey. Annals of emergency medicine. 63(6):713-20.e1. 2014. [pubmed]
Just in time for the new interns, we review our favorite resources to use on shift.
Free Open Access Medical Education (FOAM) exists in forms that are suitable for self-study or function as resources and those that are easy to use resources to consult on shift, Just In Time (JIT) Resources.
Analgesia first. Try a hydromorphone 1mg push while you’re waiting for the fentanyl drip. The endotracheal tube is uncomfortable.
Minimize sedation. There’s this principle: eCASH: early Comfort using Analgesia, minimal Sedatives and maximal Humane care [1].
Sedation: go for dexmedetomidine if you have it (but it’s expensive) or propofol. This is supported by the Society of Critical Care Medicine (SCCM) Pain, Agitation, and Delirium guidelines [2].
Be careful with rocuronium. The long duration of rocuronium means that you can’t assess for pain or discomfort so you must be responsible and get these
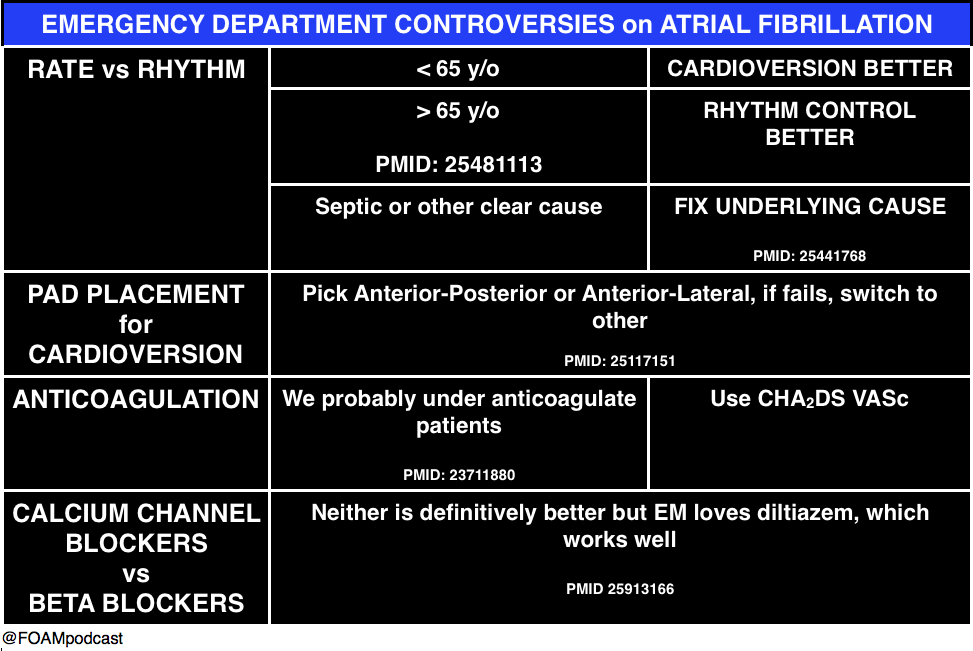
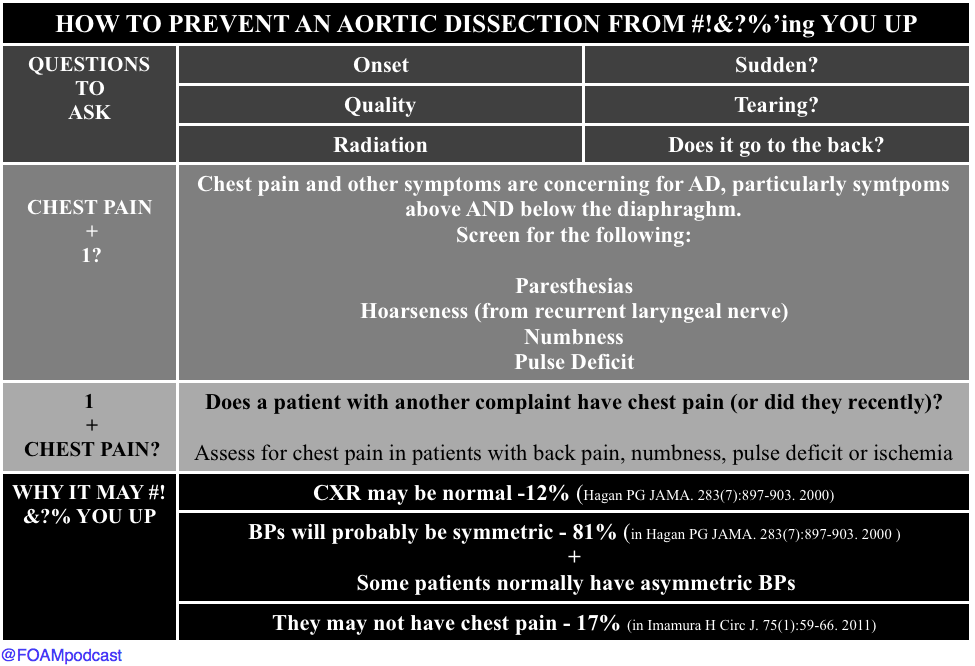
Dr. David Carr – “The Aorta Will #!&?% You Up”
Dr. Kathleen Thomas – “Oh Sh**! They’re bombing the hospital!”
We should not need a website entitled STOPBOMBINGHOSPITALS.ORG but, unfortunately, over the past 4 years, 400 hospitals have been bombed. This passionate, wrenching talk is a “must see” and “must listen” when the free talks are released on the SMACC podcast over the course of the next year.
References
Vincent J, Shehabi Y, Walsh TS et al. Comfort and patient-centred care without excessive sedation: the eCASH concept. Intensive Care Med. 42(6):962-971. 2016. [article]
Barr J, Fraser GL, Puntillo K et al. Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Critical Care Medicine. 41(1):263-306. 2013. [article]
Watt JM, Amini A, Traylor BR, Amini R, Sakles JC, Patanwala AE. Effect of paralytic type on time to post-intubation sedative use in the emergency department. Emergency medicine journal : EMJ. 30(11):893-5. 2013. [pubmed]
Imamura H, Sekiguchi Y, Iwashita T et al. Painless Acute Aortic Dissection. Circ J. 75(1):59-66. 2011. [article]
Diercks DB, et al. Clinical policy: critical issues in the evaluation and management of adult patients with suspected acute nontraumatic thoracic aortic dissection. Ann Emerg Med. 2015 Jan;65(1):32-42.e12. PMID: 25529153.
Hagan PG, Nienaber CA, Isselbacher EM. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 283(7):897-903. 2000. [pubmed]
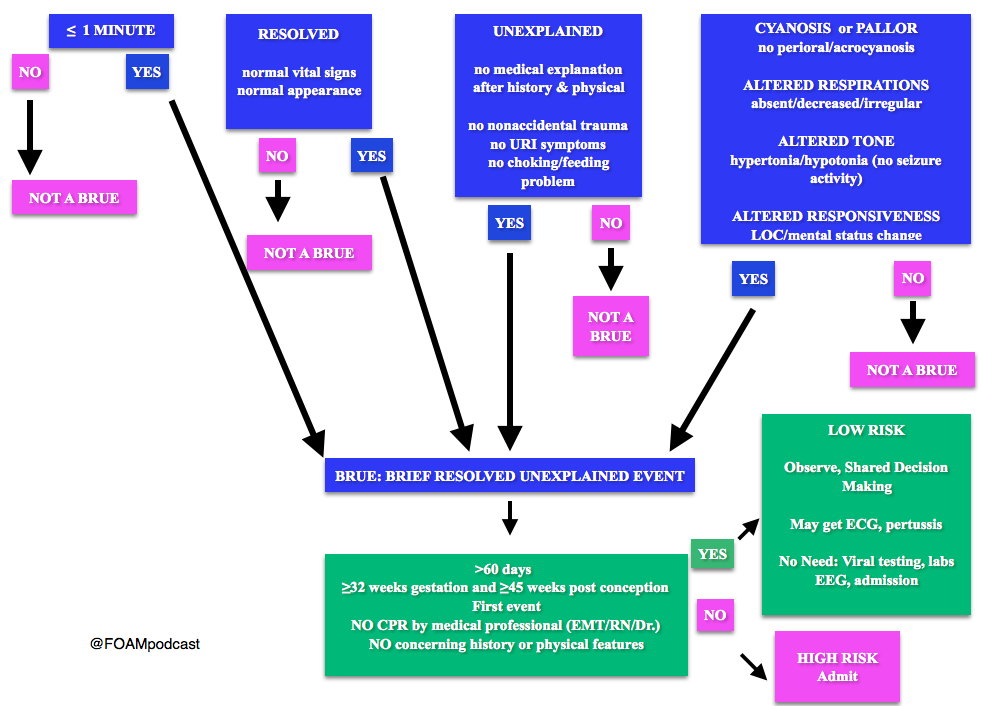
Note: Some have voiced concerns that these guidelines potentially downplay the event. The concern is that the yield of these workups and admissions may be low, but possibly worthwhile. At FOAMcast, we are not qualified to critique these guidelines but there are helpful tables and charts in them to realize that these recommendations really are only for specific events and children AFTER thorough history and physical.
Generously Donated Rosh Review Question
A 6-week-old boy is brought to the emergency room because of cyanosis. He was sleeping comfortably in a supine position right after a feeding when he suddenly choked, became limp and lips turned blue. The mother witnessed the event and blew to the face of the boy. The whole episode lasted for about two minutes. EMS was called and upon arrival at the house, the boy was back to his usual self. At the ER, he boy has normal vital signs with normal physical examination findings.
A. Admit for cardiorespiratory monitoring. The boy in the vignette had an apparent life-threatening event (ALTE) which is not a specific diagnosis but a description of an acute, unexpected episode that is frightening to the caretaker. ALTE includes one or more of the following features: apnea, color change (may be cyanotic, pallid, erythematous or plethoric), marked change in muscle tone (limpness or rigidity) and choking or gagging. A specific cause for ALTE can be identified in over one-half of patients after a careful history, physical examination, and appropriate laboratory evaluation. The remaining cases are considered idiopathic if no cause can be identified after a thorough assessment. Common etiologies for ALTE include gastroesophageal reflux, neurologic problems (such as seizures), and respiratory infection. The history of an ALTE must be taken seriously, even if the infant appears entirely well by the time he or she is evaluated. In-hospital observation with cardiorespiratory monitoring is indicated for infants whose initial evaluation suggests physiologic compromise. Hospital admission may provide important clinical information where additional episodes may be witnessed by medical personnel during the observation period. In addition, serious underlying medical conditions may become apparent. Discharging the patient after reassuring the parents (B) and observing the patient for four hours in the ER (C) are not appropriate management strategies for the infant in the vignette who needs admission for cardiorespiratory monitoring. Requesting for complete blood count (D) is not routinely done in the evaluation of an ALTE and would not aid in the management for the infant in the vignette.
We cover two bits of FOAM, one from Emergency Medicine Literature of note on the use of meclizine for vertigo and an EMcrit episode on the HiNTs exam.
Emergency Medicine Literature of Note – Dr. Ryan Radecki – Treating what you believe is peripheral vertigo?Using meclizine? So are most people.But this is not an evidence based practice. While meclizine is Rosen approved, Tintinalli recommends transdermal scopolamine as the first line treatment [1,2]. Following a recent recall of meclizine (oddly because iron bottles contained meclizine instead of iron), Dr. Radecki probes into why we use meclizine for vertigo.
Meclizine is an anti-histamine and has been thought to have anti-emetic properties.
A 1968 paper compared 16 anti-emetics/combinations and did NOT conclude that meclizine was the best. In fact, scopolamine and amphetamine performed best. Promethazine (phenergan) is also a good choice based on this paper [3].
EMcrit – Dr. Scott Weingart – The HiNTs exam has taken off, particularly in the FOAM world, as a means of disguising between central and peripheral causes of vertigo. In 2010, an EMcrit episode popularized this in the FOAM world. See this video demonstrating the HiNTs exam.
Head Impulse – rapid head rotation by the examiner with the subject’s vision fixed on an object (i.e. examiner’s nose). The examiner rapidly rotates the head towards midline and the patient’s eyes should remain fixed on the target.
Abnormal (loss of fixation on target and movement of eyes away from target followed by correct saccade as patient fixates on target) = peripheral (vestibulo-ocular reflex impaired)
Normal = central
Nystagmus
Horizontal nystagmus with a unidirectional fast phase (away from affected side) = probably peripheral
Patients with horizontal nystagmus may have central pathology but may have direction-changing nystagmus (i.e. fast phase beating in one direction when looking to right and the opposite direction when looking left).
Vertical or nystagmus = central pathology
Test of Skew Patients should fixate on a target while the provider alternately covers each eye. As the cover is moved from one eye to the other, the uncovered eye must correct for the misalignment and will look up or down to focus back on the target. This slight correction is observed repeatedly as the cover is moved from one eye to the other.
Skew deviation/misalignment = probably central, often in posterior fossa abnormalities
No skew deviation= peripheral
INFARCT – Impulse Normal, Fast-phase Alternating nystagmus, and Refixation on Cover Test
Issues with HiNTs
Can only be performed on patients with continuous vertigo.
External validity is a major issue with HiNTs.
Providers – Of the 4 studies have examined the operating characteristics of HiNTs, none have used emergency providers and instead have examined how the exam performs in the hands of two neuro-ophthalmologists, neuro-otologists, and neurologists with 4 hours of specialized training in the exam. It’s unclear whether HiNTs would be reliable or valid when performed by emergency providers [4-6].
Patients – The patients examined in many of these studies have other indicators of badness on neurologic exam. In one study, patients had to have gait instability and/or truncal ataxia to enroll. Then, 76/101 (76%) of those patients had a central cause. These patients were sick and not the undifferentiated vertiginous patients we see primarily as emergency providers [4-6].
In the words of leading HiNTs expert Dr. Newman-Toker, HiNTs “requires expertise not routinely available in emergency departments.” As such, his team is piloting quantitative video-oculography to aid in diagnosis using HiNTs [7]. An Annals of Emergency Medicine review also warned that HiNTs may not be ready for emergency provider use [9].
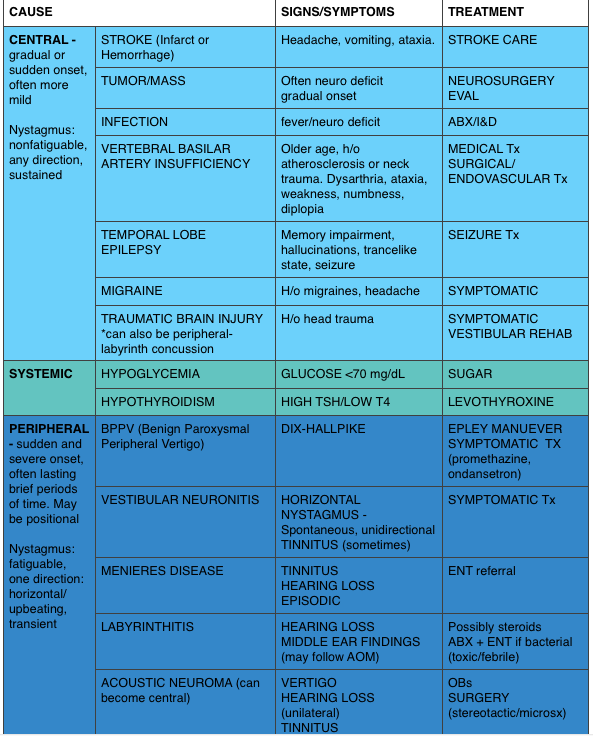
We delve into core content on vertigo using Rosen’s Medicine (8e) Chapter 19,and Tintinalli’s Emergency Medicine: A Comprehensive Study Guide(7e) Chapter 164 “Vertigo and Dizziness.”
Vertigo is often characterized by the sensation of spinning and falls into the broad and frustrating category of “dizziness.” Often, when a dizzy patient presents we perseverate on characterizes what the patient means by “dizzy.” However, some argue that this is not an appropriate approach as a study found 50% of patients changed the character of their dizziness when questioned again after 10 minutes [9]. Additionally, the clinical characteristics differentiating peripheral from central causes of vertigo are not entirely reliable. Despite these limitations, it is expected that we are familiar with “classic” presentations.
A 50-year-old man presents with episodic severe vertigo lasting hours, with associated symptoms of unilateral tinnitus, fluctuating low-frequency hearing loss, and aural fullness. [polldaddy poll=9245427]
A 20-year-old woman presents with an acute onset of dizziness. The patient describes the sensation that the room is spinning when she turns her head to the left and it is accompanied by nausea and vomiting. The symptoms resolve with turning her head away from that side. Examination reveals nystagmus elicited by deviating the eyes to the left and no other neurologic findings. [polldaddy poll=9245971]
Answers
1. B. Meniere’s disease is characterized by episodic severe vertigo lasting hours, with associated symptoms of unilateral tinnitus, fluctuating low-frequency hearing loss, and aural fullness. Typical onset is in the fifth decade of life. The cause is uncertain but is speculated to result from allergic, infectious, or autoimmune injury. The histopathologic finding includes endolymphatic hydrops, which is thought to be caused by either overproduction or underresorption of endolymph in the inner ear. Meniere’s disease is a clinical diagnosis mostly based on history. Testing may be obtained to support the diagnosis and rule out other disorders. Audiometry often demonstrates a low-frequency sensorineural hearing loss. An FTA-ABS test may be obtained to rule out syphilis. Electronystagmography (ENG) may demonstrate a unilateral peripheral vestibular weakness on caloric testing. When the diagnosis is uncertain, a brain MRI with contrast is obtained to evaluate for a retrocochlear lesion. The differential diagnosis of Meniere’s disease includes acute labyrinthitis, neurosyphilis, labyrinthine fistula, autoimmune inner ear disease, vestibular neuronitis, and migraine-associated vertigo.The most common cause of peripheral vestibular vertigo in adults is benign paroxysmal positional vertigo (A). BPPV occurs in all age groups but more often between ages 50 and 70 but is not associated with hearing loss and made worse with movement. In a perilymph fistula (C) rapid changes in air pressure (barotrauma), otologic surgery, violent nose blowing or sneezing, head trauma, or chronic ear disease may cause leakage of perilymph fluid from the inner ear into the middle ear and result in episodes of vertigo. Associated signs and symptoms are variable but can include a sudden pop in the ear followed by hearing loss, vertigo, and sometimes tinnitus. Acute vertigo associated with nausea and vomiting (but without neurologic or audiologic symptoms) that originates in the vestibular nerve is known as vestibular neuronitis (D). Vestibular neuronitis can occur spontaneously or can follow viral illness.
2. B. This patient presents with peripheral vertigo most consistent with benign paroxysmal peripheral vertigo (BPPV) and should be treated with an Epley maneuver. Vertigo is defined as the sensation of disorientation in space combined with a sensation of motion. Patients typically describe a “room-spinning” sensation or the feeling of sea sickness. Vertigo can be divided into two types: central and peripheral. Central vertigo are those disorders arising from the central nervous system and include ischemic stroke, vertebrobasilar insufficiency and infectious causes (meningitis, mastoiditis, syphilis). Central vertigo is characterized by longer duration of symptoms, minimal change with position, gradual onset and multidirectional nystagmus. Peripheral vertigo includes BPPV, Meniere’s disease, Labyrinthitis and vestibular neuritis. Peripheral vertigo may have intermittent symptoms (BPPV) or continuous symptoms but should not be associated with other neurologic deficits or changes and should have unidirectional nystagmus. The symptoms in BPPV are elicited by specific movements of the head and relieved by returning the head to a neutral position. The symptoms should be acute in onset and of a short duration. In BPPV, the symptoms are cause by the presence of an otolith in one of the semicircular canals. Although pharmacologic intervention may be necessary in the acute setting with meclizine or benzodiazepines, the best treatment for BPPV is the Epley maneuver. The Epley maneuver is a series of positions that the clinician takes the patient through that leads to expulsion of the otolith from the semicircular canal and relief of symptoms. Imaging with a non-contrast head CT (C) is not indicated in peripheral vertigo of any cause as the patient’s pathology is in the inner ear and not the brain. If a central cause is suspected, MRI of the brain (A) is the best test for diagnosis as the causative lesion will likely be in the posterior fossa, which is not seen well on CT scan. Steroid treatment (D) is the indicated management for vestibular neuritis but does not play a role in the treatment of BPPV.
References:
Chang AK, Olshaker AS. Dizziness and Vertigo. In: Marx JA, Hockberger RS, Walls RM eds. Rosen’s Emergency Medicine, 8th e.
Goldman B. Chapter 164. Vertigo and Dizziness. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds.Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011.
Cohn B. Can Bedside Oculomotor (HINTS) Testing Differentiate Central From Peripheral Causes of Vertigo? Annals of Emergency Medicine. 64(3):265-268. 2014.
Strupp M, Zingler VC, Arbusow V et al. Methylprednisolone, Valacyclovir, or the Combination for Vestibular Neuritis. N Engl J Med. 351(4):354-361. 2004.