(iTunes or listen here)
The Free Open Access Medical Education (FOAM)
We review Dr. Amal Mattu’s episode, Why You Should Care When Things are Totally RAD, on his fabulous weekly ECG video series. This week’s episode reviews Rightward Axis Deviation (RAD) and the two “can’t miss” causes in the Emergency Department (ED): Sodium channel blocker toxicity (tricyclic antidepressants and cocaine) and pulmonary hypertension (pulmonary embolism).
Causes of Rightward Axis Deviation – Lead misplacement, Hyperkalemia (can do anything on the ECG)
Ventricular ectopy (VT), Lateral MI (Q-waves in lead I), Left posterior fascicular block, Right ventricular hypertrophy, Dextrocardia
Sodium Channel Blocker Toxicity ECG clues:
- Tachycardia (most common)
- Right Axis Deviation
- Tall R wave in aVR
- Tall R in V1
- Prolonged QRS
- Prolonged QTc
EMCrit Episode 98 – Dr. Scott Weingart reviews the treatment of tricyclic antidepressant (TCA) toxicity. Top pearls
- When using sodium bicarbonate (NaHCO3) to treat TCA toxicity, the pH doesn’t seem to rise above 7.5 (but you still have to check it). Ventilate these patients appropriately (given breakdown of NaHCO3 to CO2).
- When infusing NaHCO3, check a VBG every hour to follow the pH and the potassium.
- Calcium can be critically low in these patients, replete and check accordingly.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 171 ; Rosen’s 8(e) Chapter 151, Goldfrank’s Toxicology Chapter 73 but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Tricyclic Antidepressants
Includes drugs like amitriptyline, nortriptyline and work on a variety of receptors. Other drugs, such as carbemazepine and cyclobenzaprine demonstrate TCA-like properties, albeit with different toxicologic properties (ALiEM post) Properties include anticholinergic, antihistamine, and alpha-1 adrenergic blockade in addition to sodium channel blockade and inhibition of the reuptake of norepinephrine and serotonin.
Clinical Presentation
- Anticholinergic Symptoms predominate early on – tachycardia, flushed/dry skin, mydriasis, altered mental status, urinary retention (Mad as a Hatter, Hot as a Hare, Dry as a Bone, Blind as a Bat)
- Mumbling speech
- Seizures and ventricular dysrhythmias typically occur within the first few hours after ingestion.
Diagnosis – serum TCA levels and urine drug screens have no value in acute treatment (that’s per Rosen) [2]. In addition to history and physical examination, the ECG may be helpful:
- QRS >100 ms*
- Tall R wave in lead aVR (>3mm), R/S(avr) > 0.7
- T40-ms axis between 120° and 270° (difficult to measure)
*It is widely taught, included in Rosen’s, Tintinalli, and Goldfrank, that seizures occur with a QRS >100 ms and ventricular dysrhythmias occur with a QRS >160 ms [1-3]. A 2004 meta-analysis demonstrated operating characteristics that were less than favorable, with the following characteristics:
- QRS duration >100 ms to predict seizure: Sensitivity 69% (CI 57-78), +LR 3.18, -LR 0.38
- QRS duration to predict ventricular dysrhythmia: Sensitivity 79% (CI 58-91), +LR 1.77, – LR 0.39
- Note: It appears the studies in this analysis used a QRS of 100 ms whereas traditional teaching references 160 ms as the threshold for most ventricular dysrhythmias
- Most predictive of ventricular dysrhythmia: R/S waves ratio (+LR 15.67) but this was evaluated in only one study (Sensitivity 47%)
[4]
Treatment
In acute overdose with an ingestion < 1 hour prior, activated charcoal may be given if no contraindications exist.
Symptomatic treatment and observation for at least six hours.
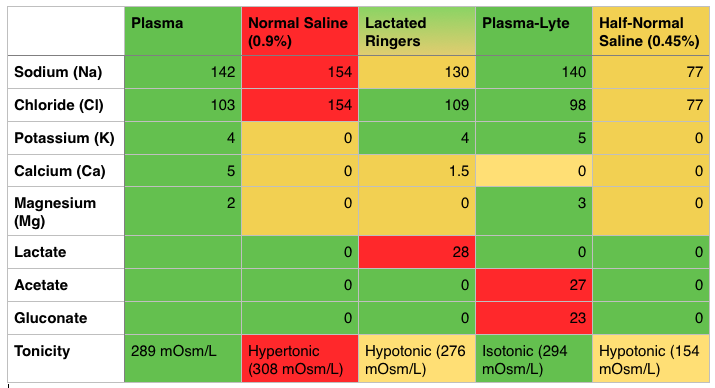
Hypotension – crystalloid intravenous fluids, vasopressors if needed (norepinephrine)
Seizure – Most seizures are self-limiting and spontaneously terminate within 3 minutes but benzodiazepines and standard seizure treatment can be used .
Prolonged QRS (>100 ms) or Dysrhythmia
Sodium Bicarbonate – 1-2 mEq/kg bolus. Each amp of NaHCO3 has 50 mEq so the average 70 kg patient can get 1.5-2.5 amps. An infusion of NaHCO3 may be used (3 amps of NaHCO3 in 1 L of D5W).
- Caution: must follow pH (can titrate as high as 7.5-7.55) as well as potassium.
If the NaHCO3 pushes the patient’s pH to the 7.5-7.55 limit and the QRS remains wide, 200 mL of hypertonic saline (3%) can be used.
Lidocaine, a class IB sodium channel blocker/antiarrhythmic can also be used although it may seem counterintuitive.
Magnesium may also be used
Disposition:
Asymptomatic patients six hours after ingestion (no sinus tachycardia) can be medically cleared.
Generously Donated Rosh Review Questions (Scroll for Answers)
Question 1. A 24-year-old man presents to the ED via the police because of altered mental status and violent behavior. The patient reportedly had been on a drug binge, using amphetamines and cocaine for the last 2 days. On arrival, he is afebrile, his heart rate is 140 beats per minute, blood pressure is 180/110 mm Hg, and he is respiring at 22 breaths per minute. He is agitated and combative, but there is no evidence of traumatic injury. His pupils are dilated, and he is diaphoretic. Which of the following statements is true regarding the treatment of amphetamine and cocaine toxicity?
A. Antipsychotics are the preferred initial therapy for agitation and psychosis
B. Beta-adrenergic blockers are safe for managing tachycardia and dysrhythmias
C. Body packers with leaking packets should receive whole-bowel irrigation
D. Vasodilators are first-line therapy for treating amphetamine-induced hypertension
E. Wide-complex tachydysrhythmias should be treated initially with sodium bicarbonate
Question 2. A 27-year-old man is brought to the ED by EMS after being found wandering in the street. His BP is 155/70, HR 115, T 37.5°C, RR 16, pulse ox 99% on room air, and finger stick glucose 98. On exam, the patient is confused with mumbling speech. His pupils are 7 mm and reactive. His face is flushed. Mucous membranes and skin are dry. Which of the following toxidromes is this patient exhibiting?
A. Anticholinergic
B. Cholinergic
C. Sedative-hypnotic
D. Sympathomimetic
More FOAM:
Life in the Fast Lane TCA case
Life in the Fast Lane TCA ECG
References:
1. Chapter 151. Rosen’s Emergency Medicine, 8e.
2.Chapter 171. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
3.Chapter 73. Goldfrank’s Toxicologic Emergencies, 9e, 2010
4. Bailey B, Sc M. A Meta-Analysis of Prognostic Indicators to Predict Seizures , Arrhythmias or Death After Tricyclic Antidepressant Overdose . 2004;42(6):877–888. doi:10.1081/CLT-200035286.