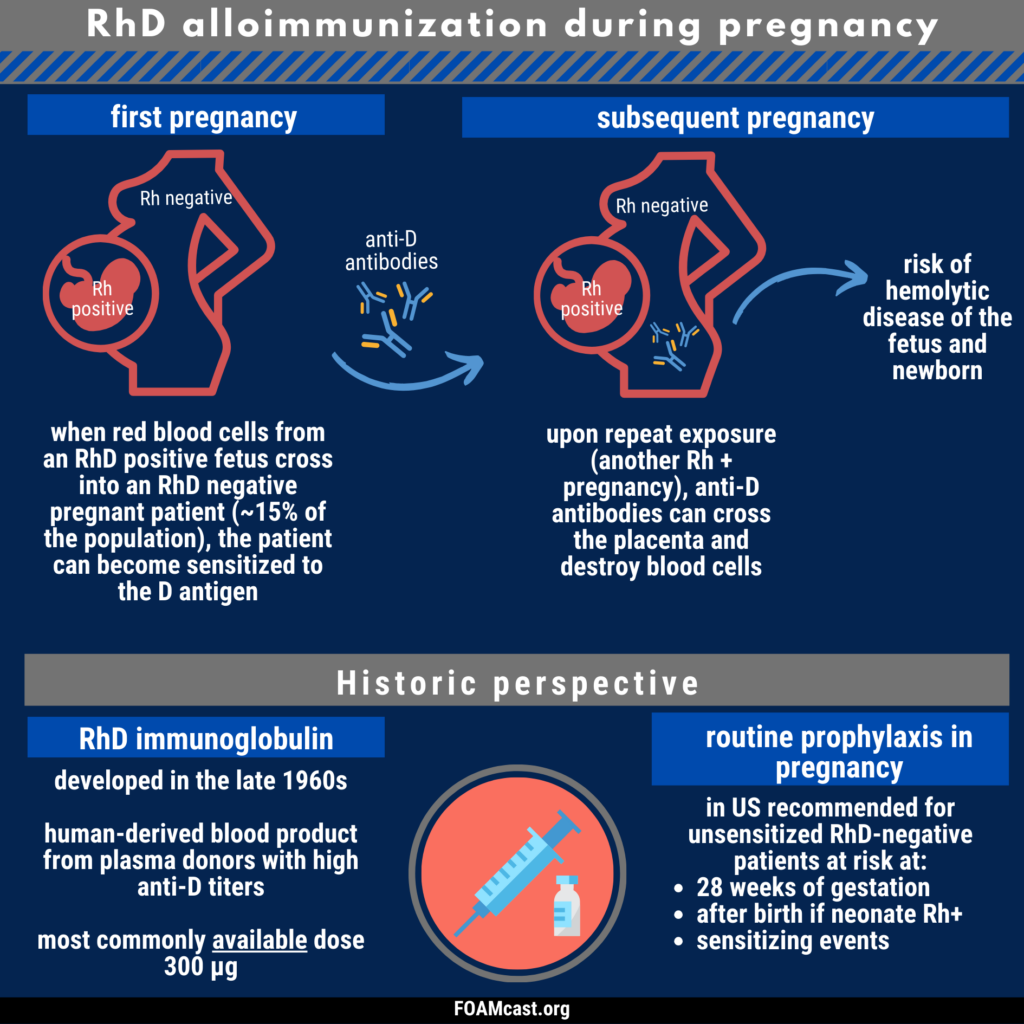
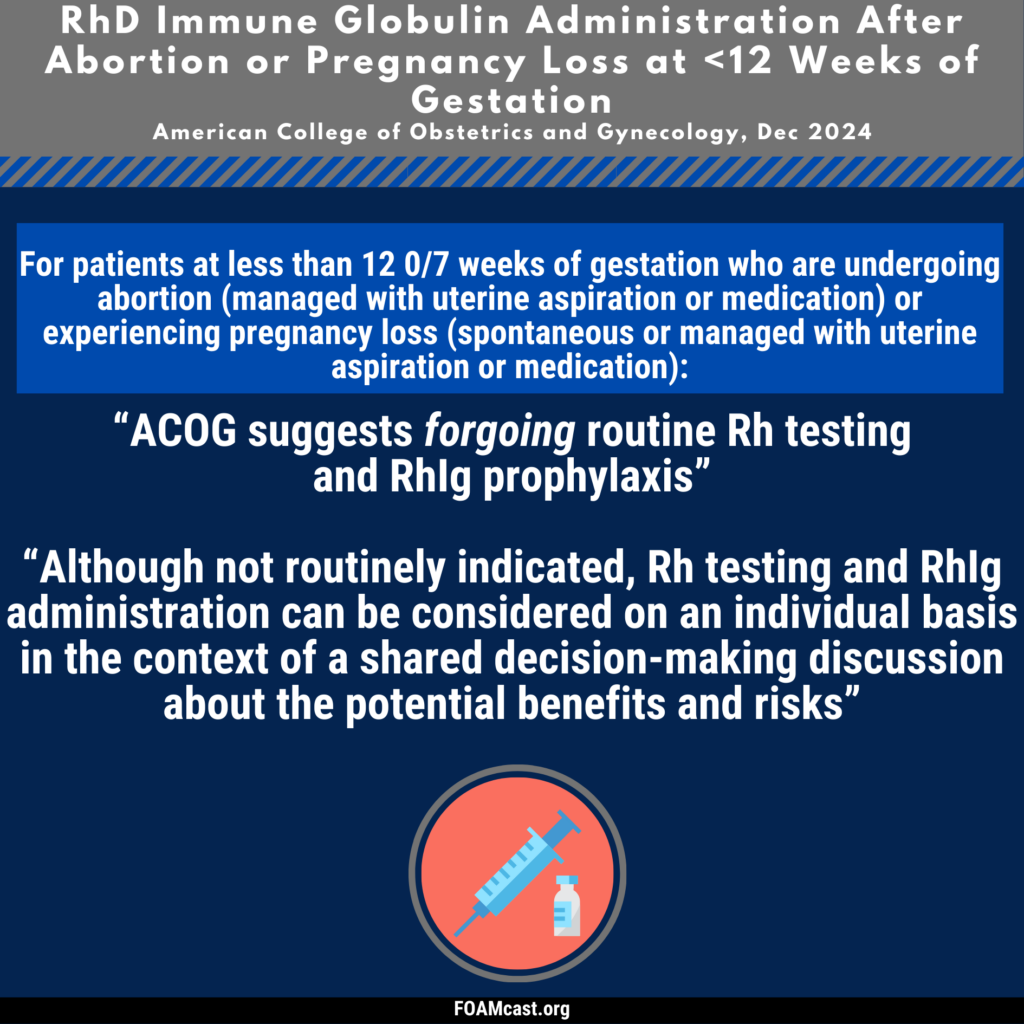
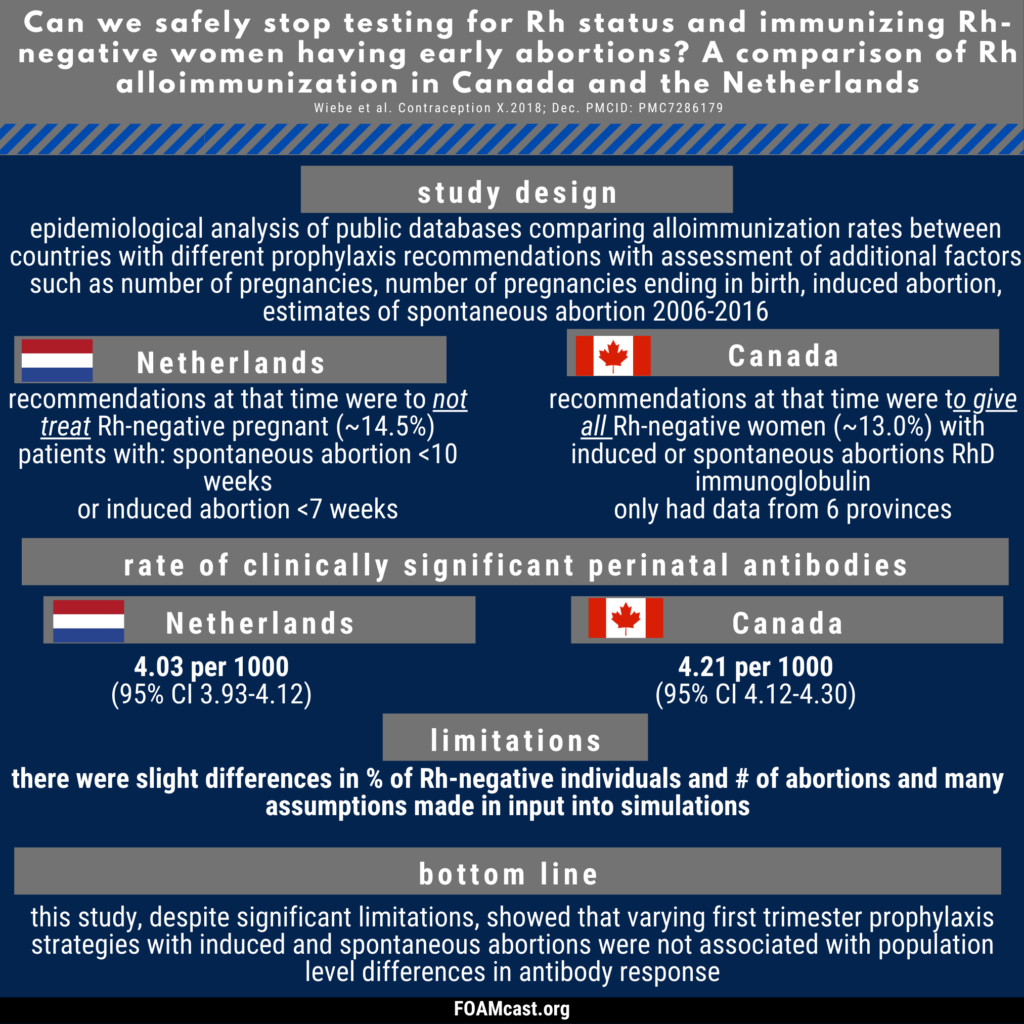
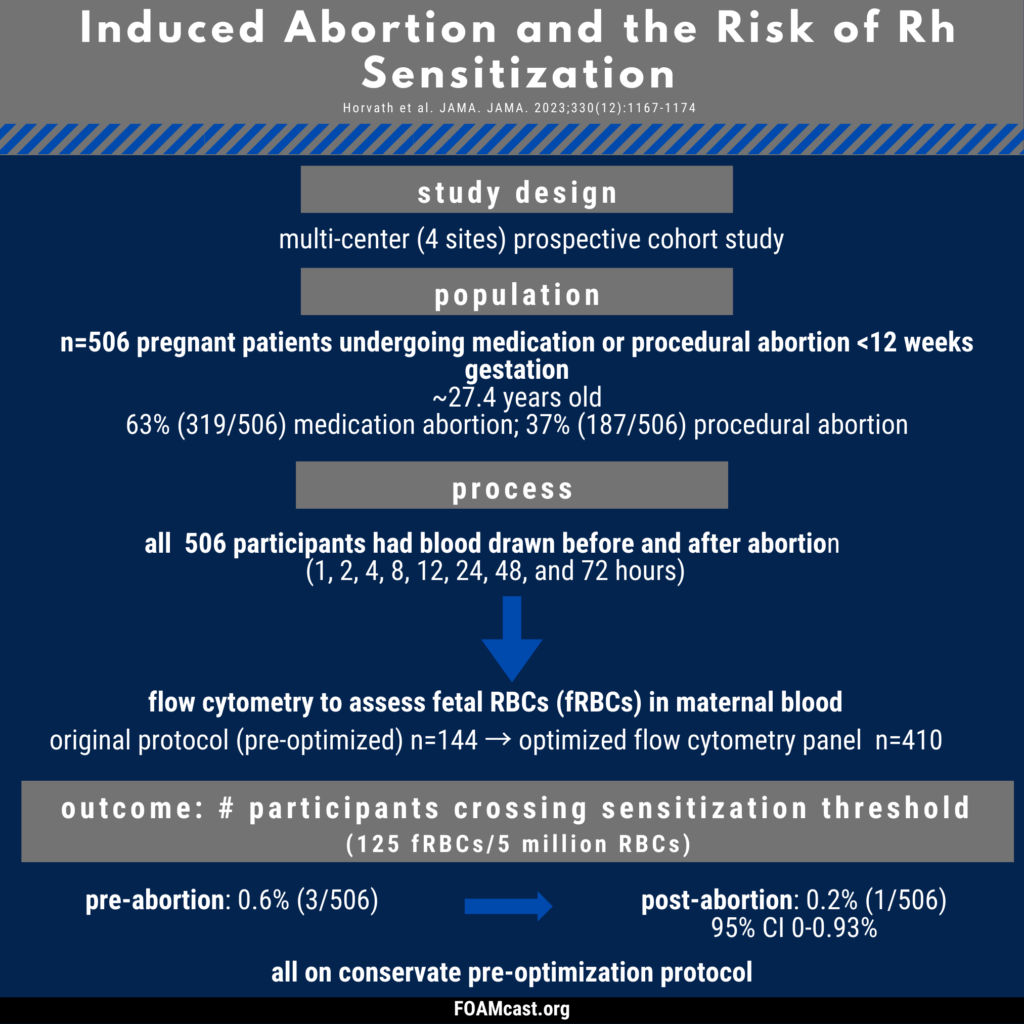
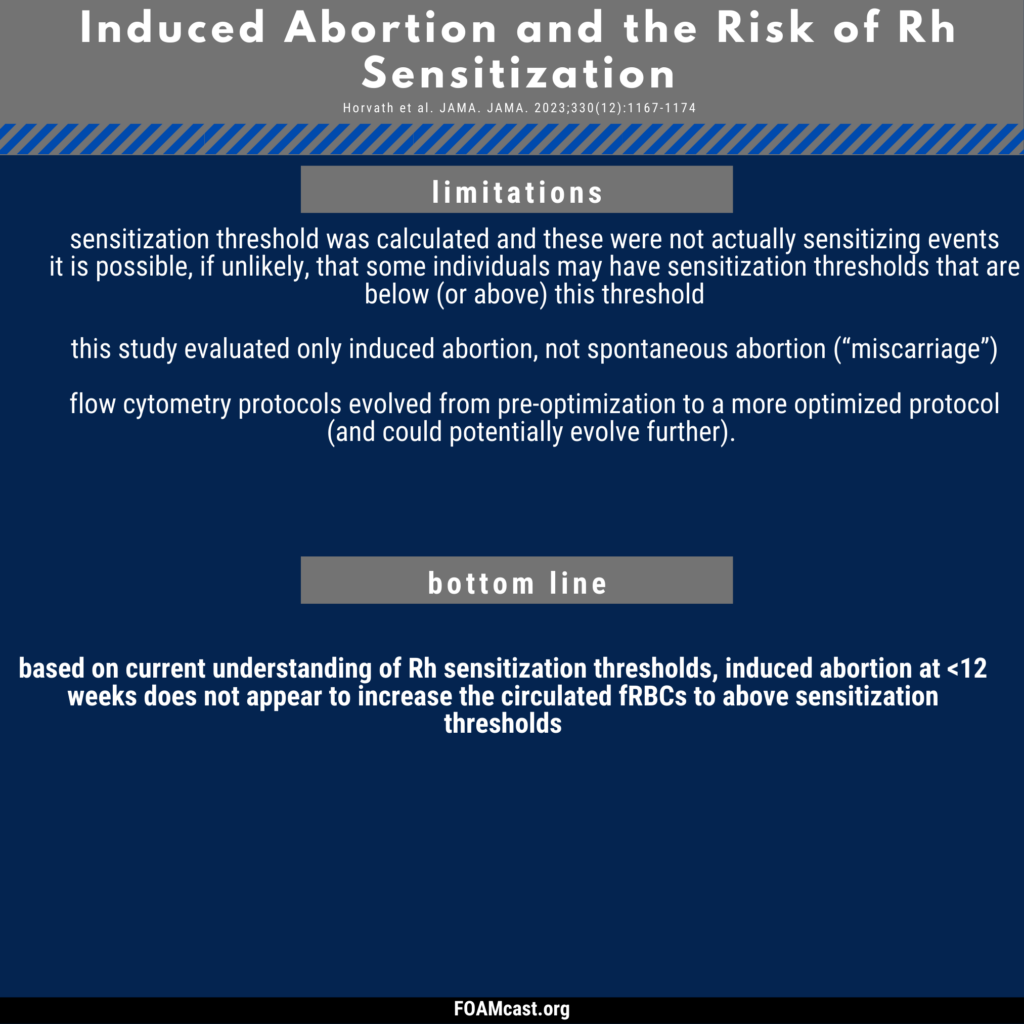
Historically, care of patients in the emergency department (ED) in the first trimester with any kind of abortion (e.g. spontaneous “miscarriage”) underwent blood type and Rh testing followed by RhD immunoglobulin prophylaxis if Rh+. However, many guidelines now recommend foregoing this process in first trimester abortion (spontaneous or induced). In this episode, we dive into the evidence behind these varying recommendations.
The paper: The authors took blood samples from 760 healthy pregnant patients at one point during their pregnancy. They propose a continuous increase for a normal d-dimer cut off throughout gestation.
1-12 weeks: n=33, 81% with normal d-dimer
19-21 weeks: n=53, 32% with normal d-dimer
28-36 weeks: n=8, 6% with normal d-dimer
39-40 weeks: 0, 0% normal d-dimer
Postpartum day 2: n=12, 8% with normal d-dimer
Dr. Radecki’s “Take Home:“
Dr. Kline has advocated for the following d-dimer cut offs in pregnancy: 1st trimester 750 ng/mL, 2nd trimester 1000 ng/mL, and 3rd trimester 1250 ng/mL(based on a standard cut-off of 500 ng/mL) and this may be reasonable but is not rooted in robust evidence.
Interestingly, this post was followed by another post covering an article by Hutchinson et al from Am J Roentgenol showing that of 174 CTPAs initially read as positive, 45 were read as negative by chest radiologist upon blinded retrospective review. That means 25.9% of this cohort diagnosed with PE apparently had negative CT scans.
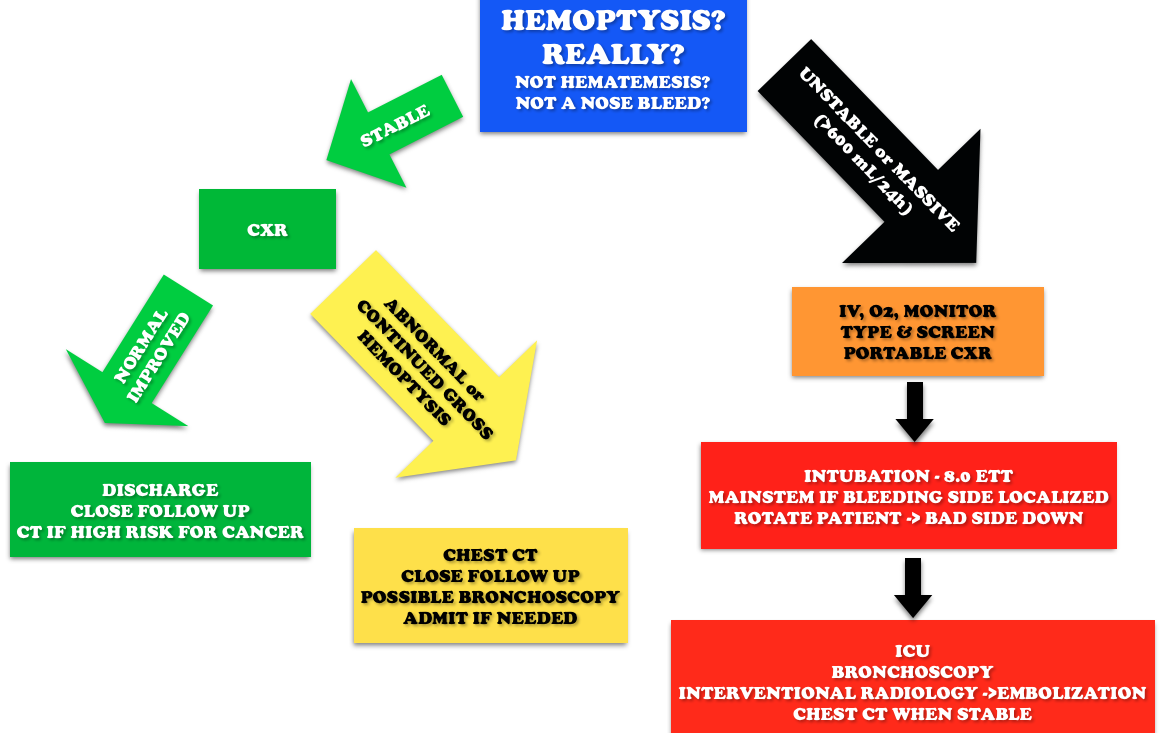
Core Content – Hemoptysis
Tintinalli (7e) Chapter 66; Rosen’s Emergency Medicine (8e) Chapter 24
Etiology: Most common causes are bronchitis (often blood tinged sputum), infection (abscess, pneumonia, tuberculosis), neoplasm (lung cancer). Other causes include iatrogenic causes (bronchoscopy, biopsy, aspirated foreign body), anticoagulation, and autoimmune diseases such as granulomatous polyangiitis (Wegener’s), lupus, and Goodpasture’s.
Question 1. A 50-year-old man, nonsmoker, presents to the ED with a 2-day history of cough now associated with frank hemoptysis. He denies any constitutional symptoms. Vital signs are BP 125/70, HR 80, RR 16, and pulse oximetry is 98% on room air. On exam, his lung fields are clear; the remainder of the exam is unremarkable. A chest radiograph is performed, which is normal. [polldaddy poll=9039260]
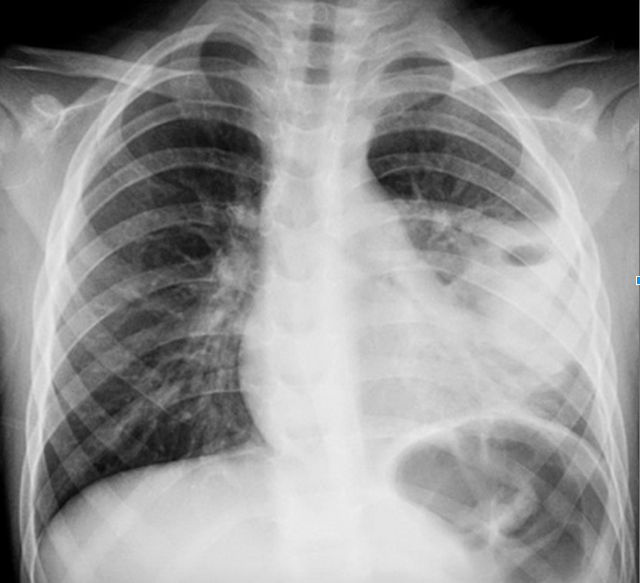
Question 2. A 55-year-old man, smoker, presents to the ED with hemoptysis and dyspnea for 4 weeks. His VS are T 37°C, BP 146/76 mm Hg, HR 85 bpm, RR 20 per minute, and oxygen saturation 96% on RA. His lung exam reveals distant breath sounds on the left side. His chest X-ray is shown below. [polldaddy poll=9039262]
Rosh Review
Answers
1.C. The patient is hemodynamically stable with a normal chest radiograph, so he does not require ICU admission (A). Patients with massive hemoptysis require ICU admission. The decision to perform a bronchoscopy (B) in this patient will be left up to the pulmonologist. Given the overall clinical picture, urgent bronchoscopy is not required in this case. With massive hemoptysis, an emergent bronchoscopy is indicated. Bronchitis (D) typically presents with the abrupt onset of cough with blood-streaked purulent sputum. The patient in the clinical scenario has persistent frank hemoptysis, which mandates further investigation. In a patient who does not smoke, is under the age of 40, and has a normal chest radiograph and scant hemoptysis, treatment for bronchitis can be initiated with outpatient follow-up.
2. B. Although bronchitis (A) is the most common cause of hemoptysis (responsible for 15%-30% of cases), patients present with cough as the dominant symptom and have abnormal lung exams and normal chest x-rays. The cough may be productive of sputum. The diagnosis of pneumonia (C) requires focal findings on physical exam or infiltrates on radiographic imaging and is typically accompanied by a fever. Patients with lung cancer are at increased risk for pulmonary embolism (D). This patient’s Wells score is 2 (one point each for hemoptysis and malignancy), which makes the likelihood of PE 16% in an ED population. Given the lung mass seen on chest x-ray, lung cancer is more likely than PE.
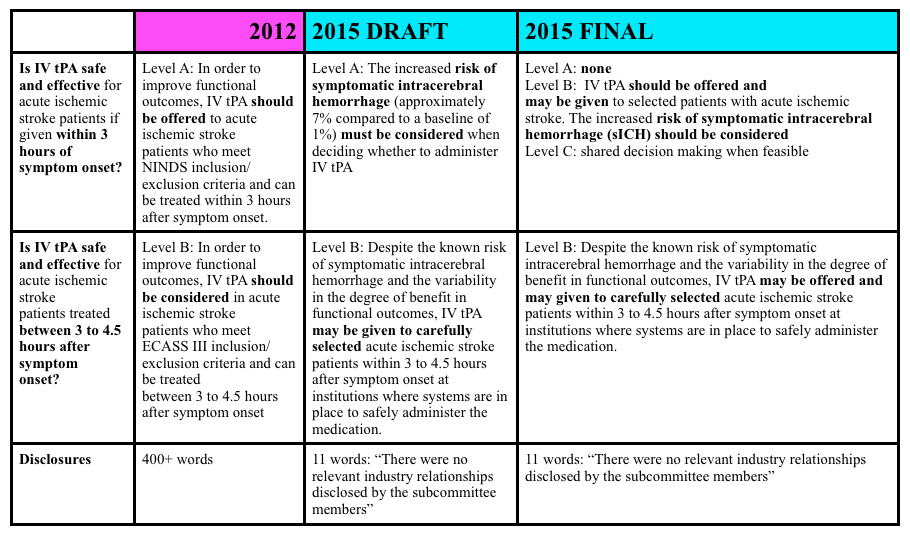
NNT of 8 for excellent functional outcomes; 95% [CI] 4-31
Paucity of patients presenting with mild stroke (NIHSS score 0 to 4)
NNH of 17 for symptomatic intracerebral hemorrhage; 95% CI 12-34
While FOAMcast is not an interview style podcast, we felt compelled to get some perspective on Emergency Physicians a little more experienced than ourselves. Here we interview:
Dr. Ryan Radecki (@emlitofnote), Assistant Professor, University of Texas – Houston
No clear cut winner in the beta-blocker vs. calcium channel blocker battle
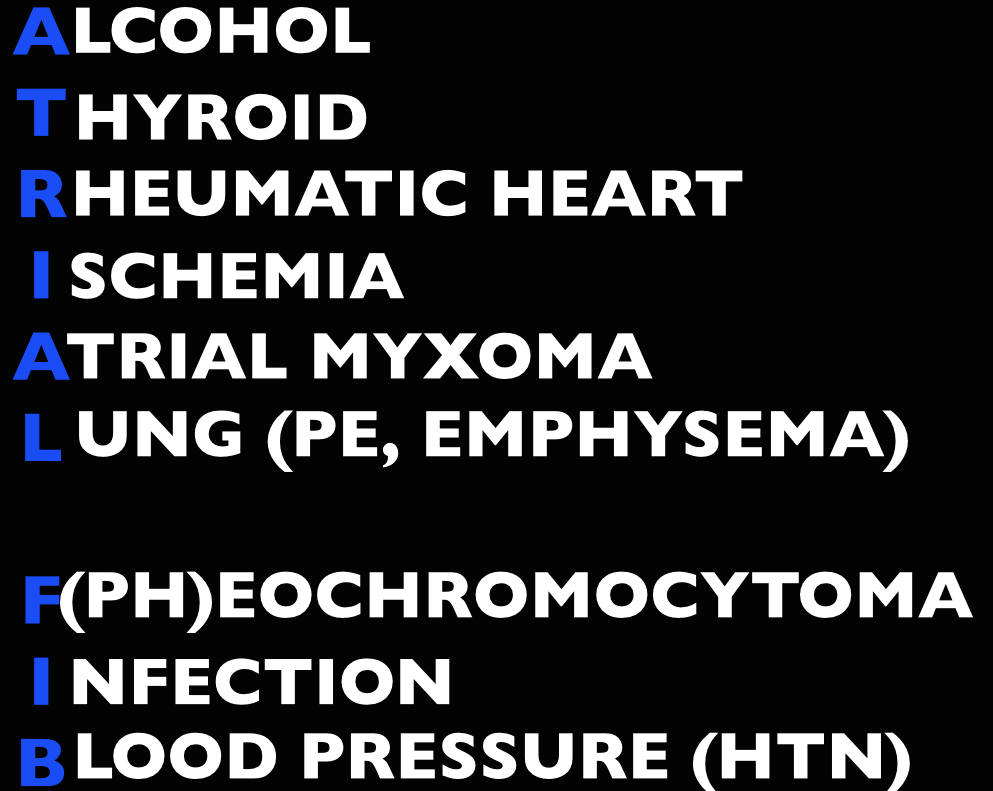
Long Term Atrial Fibrillation Management in General:
Avoid beta-blockers in:
Obstructive lung disease (asthma/COPD)
Peripheral vascular disease
Diabetics
Severe congestive heart failure (CHF)
Erectile dysfunction
Avoid calcium-channel blockers in:
Severe CHF and acute decompensated heart failure (ADHF)
Of note, in patients
The Maryland Critical Care Project has a great post with many of Dr. Amal Mattu’s key FOAM talks embedded on Tachydysrhythmias You Gotta Know.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 280, 295 ; Rosen’s 8(e) Chapter 50 – a well written chapter, but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Pads in either an anterior-lateral (AL) or anterior-posterior (AP) position followed by synchronized cardioversion at 100-200 J biphasic. Current literature shows no significant difference in pad placement [1]
Rate control. A target of <120 beats per minute is acceptable in the ED [2-3]. First line agents are nodal blocking agents such as diltiazem and metoprolol
Diltiazem 0.25 mg/kg IV over 2 minutes with a peak effect in 2-7 minutes. Can repeat at 0.35 mg/kg IV over 2 minutes.
Metoprolol 5-10 mg IV.
Rhythm control with cardioversion. While there’s no proven benefit to rhythm control, many patients would prefer to be in sinus rhythm and ED cardioversion of stable new-onset atrial fibrillation is appropriate in a select population, notably, when the onset is <48 hours (or <72 hours per Rosen). The pooled literature suggests a thromboembolism rate <0.8% [4].
Note: A recent article in JAMA by Nuotio et al found a higher rate of embolic events in patients who were electively cardioverted after >12 hours in atrial fibrillation.The 30 day risk of thromboembolism when cardioverted between 12-48 hours was 1.1%, compared to the ~2% risk if cardioverted after 48 hours. While the risk is still small, it is higher than the ~0.3% risk of thromboembolism with anticoagulation on board.
Treat the underlying cause (ex: sepsis, pulmonary embolism, hyperthyroidism, etc)
May also consider Amiodarone, Digoxin (mean >11 hours to rate control) [3]
In atrial fibrillation with pre-excitation (WPW), an often wide and irregular rhythm with different/changing morphologies to the QRS do NOT treat with an AV Nodal blocking agent as this may result in death (Adenosine, Beta-blocker, Calcium-channel blocker, etc). Treat with procainamide or shock
Disposition – Admit patients that present unstable, with underlying co-morbidities, or those that are not rate controlled. Depending on the patient’s follow up and local practice patterns, the
More sensitive to electrical cardioversion, less sensitive to chemical cardioversion
Multifocal Atrial Tachycardia
Irregular narrow complex tachycardia with p waves of at least 3 morphologies (this can be difficult to see, so look in multiple leads, particularly V2)
Etiology -often seen in advanced pulmonary disease
Management – Treat the underlying cause, do NOT cardiovert MAT
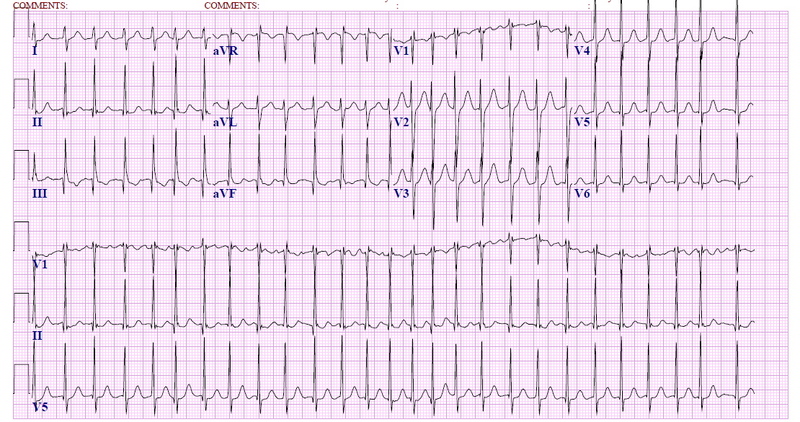
Question 1. A 72-year-old man with a history of hypertension, diabetes, and congestive heart failure presents to the ED with heart palpitations for the past 4 days. He denies any chest pain, shortness of breath, abdominal pain, or history of similar palpitations. In the ED, his vital signs are BP 135/75, HR 138, RR 14, and oxygen saturation 98% on room air. His ECG is seen below. Which of the following is the most appropriate next step in management?
Rosh Review
A. Chemical cardioversion
B. Rate Control
C. Synchronized cardioversion
D. Warfarin
Question 2. When do you worry about giving calcium channel blockers, beta-blockers, or digoxin in a patient with atrial fibrillation?
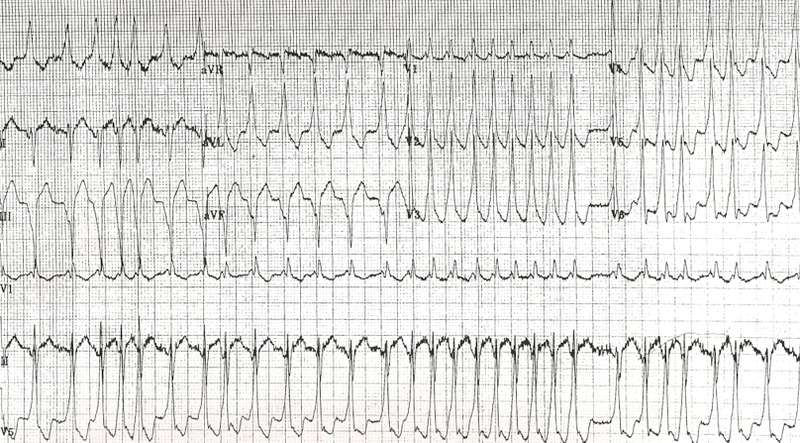
Question 3. An 18-year-old woman presents with palpitations and near syncope. Her vitals are T 98.7F, HR 199, BP 113/66, RR 32, and oxygen saturation 94%. Her ECG is shown below. What treatment is indicated?
Rosh Review
A. Administer adenosine 6 mg IV
B. Administer diltiazem 10 mg IV
C. Administer lopressor 10 mg IV
D. Administer procainamide 100mg IV
References
1. Kirkland S, Stiell I, AlShawabkeh T, Campbell S, Dickinson G, Rowe BH. The Efficacy of Pad Placement for Electrical Cardioversion of Atrial Fibrillation/Flutter: A Systematic Review. Acad Emerg Med. 2014;21(7):717–726.
2. Chapter. Rosen’s Emergency Medicine, 8e.
3.Chapter. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
4. Cohn BG, Keim SM, Yealy DM. Is Emergency Department Cardioversion of Recent-onset Atrial Fibrillation Safe and Effective? J Emerg Med. 2013;45(1):117–27.
Answers
1. B. Atrial fibrillation is caused by chaotic, disorderly firing from a second focus within the atria, resulting in uncoordinated atrial contractions. Patients with atrial fibrillation may present with palpitations, chest pain, shortness of breath, or they may be asymptomatic. Atrial fibrillation can be classified as chronic or paroxysmal, with paroxysms lasting minutes to days. On ECG, there are irregularly irregular narrow QRS complexes. In addition, no discernible p-waves are noted, rather fibrillatory waves are seen. Unless the patient is hemodynamically unstable, the mainstay of therapy is rate control. This is achieved through medications that act on the AV node such as calcium channel blockers (eg diltiazem or verapamil), beta-blockers, or digoxin. Due to digoxin’s slow onset of action and side effects, it is considered a second line medication.
If atrial fibrillation has been present for >48 hours, there is an increased risk of atrial thrombus formation. An echocardiogram should be obtained in these patients to exclude thrombus formation prior to rhythm control. Patients with chronic atrial fibrillation usually are placed on warfarin (D) or a similar anticoagulant to prevent thromboembolism.Chemical cardioversion (A) (amiorodone, procainamide or flecainide) can be attempted in patients with paroxysmal atrial fibrillation for less than 48 hours. Synchronized cardioversion (C) is used in patients who are hemodynamically unstable. This can be achieved by administering 50 – 100 J of electricity in synchronization mode.
2. If a patient has an accessory pathway, such as Wolff-Parkinson-White Syndrome.
3. D. This patient presents with near syncope in the setting of atrial fibrillation with abberant conduction most likely secondary to Wolff-Parkinson-White (WPW) syndrome and should be chemically or electrically cardioverted. WPW syndrome refers to the presence of an accessory pathway between the right atrium and right ventricle. This accessory pathway has a shortened refractory period and can bypass normal conduction down the AV node. Because of the shortened refractory time, the accessory pathway in WPW can conduct atrial impulses much faster than the AV node can allowing for a ventricular rate between 150 and 300 beats per minute. Any tachycardia greater than 200 beats per minute in an adult should raise suspicion for an accessory pathway.
Patients with WPW can be asymptomatic or may present with severe tachydysrhythmias. The most common presenting dysrhythmia is reentrant tachycardia (70-80%) and second is atrial fibrillation (10-30%). In these tachydysrhythmias, the patient can conduct orthodromically (down the AV node and back up the accessory pathway), antidromically (down the accessory pathway and up the AV node) or in both directions. Patients who have any antidromic conduction will present with wide complex tachycardias. In patients with irregularly irregular wide-complex tachycardias, atrial fibrillation with WPW is the most common diagnosis. If the patient is unstable, electrical cardioversion should be pursued immediately as these patients run the risk of degrading into ventricular tachycardia and ventricular fibrillation. If the patient is stable, procainamide can be administered for chemical cardioversion. Procainamide is a class Ia anitdysrhythmic agent. The dose of procainamide (D) is 18-20 mg/kg administered at a rate of 20-30 mg/min.
In patients with WPW, antidysrhythmic agents that block the AV node are contraindicated. Blocking the AV node causes unopposed electrical conduction down the accessory pathway. This can lead to ventricular dysrhythmias. Additionally, the accessory pathway in WPW responds paradoxically to AV nodal blocking agents by further decreasing its refractory time. Adenosine (A), beta-blockers (C), calcium-channel blockers (B) and digoxin all block the AV node.
No clear cut winner in the beta-blocker vs. calcium channel blocker battle
Long Term Atrial Fibrillation Management in General:
Avoid beta-blockers in:
Obstructive lung disease (asthma/COPD)
Peripheral vascular disease
Diabetics
Severe congestive heart failure (CHF)
Erectile dysfunction
Avoid calcium-channel blockers in:
Severe CHF and acute decompensated heart failure (ADHF)
Of note, in patients
The Maryland Critical Care Project has a great post with many of Dr. Amal Mattu’s key FOAM talks embedded on Tachydysrhythmias You Gotta Know.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 280, 295 ; Rosen’s 8(e) Chapter 50 – a well written chapter, but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Pads in either an anterior-lateral (AL) or anterior-posterior (AP) position followed by synchronized cardioversion at 100-200 J biphasic. Current literature shows no significant difference in pad placement [1]
Rate control. A target of <120 beats per minute is acceptable in the ED [2-3]. First line agents are nodal blocking agents such as diltiazem and metoprolol
Diltiazem 0.25 mg/kg IV over 2 minutes with a peak effect in 2-7 minutes. Can repeat at 0.35 mg/kg IV over 2 minutes.
Metoprolol 5-10 mg IV.
Rhythm control with cardioversion. While there’s no proven benefit to rhythm control, many patients would prefer to be in sinus rhythm and ED cardioversion of stable new-onset atrial fibrillation is appropriate in a select population, notably, when the onset is <48 hours (or <72 hours per Rosen). The pooled literature suggests a thromboembolism rate <0.8% [4].
Note: A recent article in JAMA by Nuotio et al found a higher rate of embolic events in patients who were electively cardioverted after >12 hours in atrial fibrillation.The 30 day risk of thromboembolism when cardioverted between 12-48 hours was 1.1%, compared to the ~2% risk if cardioverted after 48 hours. While the risk is still small, it is higher than the ~0.3% risk of thromboembolism with anticoagulation on board.
Treat the underlying cause (ex: sepsis, pulmonary embolism, hyperthyroidism, etc)
May also consider Amiodarone, Digoxin (mean >11 hours to rate control) [3]
In atrial fibrillation with pre-excitation (WPW), an often wide and irregular rhythm with different/changing morphologies to the QRS do NOT treat with an AV Nodal blocking agent as this may result in death (Adenosine, Beta-blocker, Calcium-channel blocker, etc). Treat with procainamide or shock
Disposition – Admit patients that present unstable, with underlying co-morbidities, or those that are not rate controlled. Depending on the patient’s follow up and local practice patterns, the
More sensitive to electrical cardioversion, less sensitive to chemical cardioversion
Multifocal Atrial Tachycardia
Irregular narrow complex tachycardia with p waves of at least 3 morphologies (this can be difficult to see, so look in multiple leads, particularly V2)
Etiology -often seen in advanced pulmonary disease
Management – Treat the underlying cause, do NOT cardiovert MAT
Question 1. A 72-year-old man with a history of hypertension, diabetes, and congestive heart failure presents to the ED with heart palpitations for the past 4 days. He denies any chest pain, shortness of breath, abdominal pain, or history of similar palpitations. In the ED, his vital signs are BP 135/75, HR 138, RR 14, and oxygen saturation 98% on room air. His ECG is seen below. Which of the following is the most appropriate next step in management?
Rosh Review
A. Chemical cardioversion
B. Rate Control
C. Synchronized cardioversion
D. Warfarin
Question 2. When do you worry about giving calcium channel blockers, beta-blockers, or digoxin in a patient with atrial fibrillation?
Question 3. An 18-year-old woman presents with palpitations and near syncope. Her vitals are T 98.7F, HR 199, BP 113/66, RR 32, and oxygen saturation 94%. Her ECG is shown below. What treatment is indicated?
Rosh Review
A. Administer adenosine 6 mg IV
B. Administer diltiazem 10 mg IV
C. Administer lopressor 10 mg IV
D. Administer procainamide 100mg IV
References
1. Kirkland S, Stiell I, AlShawabkeh T, Campbell S, Dickinson G, Rowe BH. The Efficacy of Pad Placement for Electrical Cardioversion of Atrial Fibrillation/Flutter: A Systematic Review. Acad Emerg Med. 2014;21(7):717–726.
2. Chapter. Rosen’s Emergency Medicine, 8e.
3.Chapter. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
4. Cohn BG, Keim SM, Yealy DM. Is Emergency Department Cardioversion of Recent-onset Atrial Fibrillation Safe and Effective? J Emerg Med. 2013;45(1):117–27.
Answers
1. B. Atrial fibrillation is caused by chaotic, disorderly firing from a second focus within the atria, resulting in uncoordinated atrial contractions. Patients with atrial fibrillation may present with palpitations, chest pain, shortness of breath, or they may be asymptomatic. Atrial fibrillation can be classified as chronic or paroxysmal, with paroxysms lasting minutes to days. On ECG, there are irregularly irregular narrow QRS complexes. In addition, no discernible p-waves are noted, rather fibrillatory waves are seen. Unless the patient is hemodynamically unstable, the mainstay of therapy is rate control. This is achieved through medications that act on the AV node such as calcium channel blockers (eg diltiazem or verapamil), beta-blockers, or digoxin. Due to digoxin’s slow onset of action and side effects, it is considered a second line medication.
If atrial fibrillation has been present for >48 hours, there is an increased risk of atrial thrombus formation. An echocardiogram should be obtained in these patients to exclude thrombus formation prior to rhythm control. Patients with chronic atrial fibrillation usually are placed on warfarin (D) or a similar anticoagulant to prevent thromboembolism.Chemical cardioversion (A) (amiorodone, procainamide or flecainide) can be attempted in patients with paroxysmal atrial fibrillation for less than 48 hours. Synchronized cardioversion (C) is used in patients who are hemodynamically unstable. This can be achieved by administering 50 – 100 J of electricity in synchronization mode.
2. If a patient has an accessory pathway, such as Wolff-Parkinson-White Syndrome.
3. D. This patient presents with near syncope in the setting of atrial fibrillation with abberant conduction most likely secondary to Wolff-Parkinson-White (WPW) syndrome and should be chemically or electrically cardioverted. WPW syndrome refers to the presence of an accessory pathway between the right atrium and right ventricle. This accessory pathway has a shortened refractory period and can bypass normal conduction down the AV node. Because of the shortened refractory time, the accessory pathway in WPW can conduct atrial impulses much faster than the AV node can allowing for a ventricular rate between 150 and 300 beats per minute. Any tachycardia greater than 200 beats per minute in an adult should raise suspicion for an accessory pathway.
Patients with WPW can be asymptomatic or may present with severe tachydysrhythmias. The most common presenting dysrhythmia is reentrant tachycardia (70-80%) and second is atrial fibrillation (10-30%). In these tachydysrhythmias, the patient can conduct orthodromically (down the AV node and back up the accessory pathway), antidromically (down the accessory pathway and up the AV node) or in both directions. Patients who have any antidromic conduction will present with wide complex tachycardias. In patients with irregularly irregular wide-complex tachycardias, atrial fibrillation with WPW is the most common diagnosis. If the patient is unstable, electrical cardioversion should be pursued immediately as these patients run the risk of degrading into ventricular tachycardia and ventricular fibrillation. If the patient is stable, procainamide can be administered for chemical cardioversion. Procainamide is a class Ia anitdysrhythmic agent. The dose of procainamide (D) is 18-20 mg/kg administered at a rate of 20-30 mg/min.
In patients with WPW, antidysrhythmic agents that block the AV node are contraindicated. Blocking the AV node causes unopposed electrical conduction down the accessory pathway. This can lead to ventricular dysrhythmias. Additionally, the accessory pathway in WPW responds paradoxically to AV nodal blocking agents by further decreasing its refractory time. Adenosine (A), beta-blockers (C), calcium-channel blockers (B) and digoxin all block the AV node.
We review RAGE Podcast Episode 4 that awesomely covers nearly everything under the sun. A few of our favorite pearls:
Impact apnea –people who sustain traumatic brain injury often have associated apnea. Support their airway because this could lead to arrest. Bystander support is crucial.
Right Ventricular Myocardial Infarction (RVMI)– Think about this in any inferior MI situation. Give fluids, these patients are preload dependent and need the cath lab.
Optimize Oxygenation, Hemodynamics, Contractility, Rate/rhythm, Afterload, and Preload
Give fluids, but not too much. Inotropes and vasopressors are often necessary. These guys like milrinone and epinephrine.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapters 53, 57; Rosen’s (8e) Chapters 78, 81…but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
RVMI – often associated with inferior MIs and can carry increased morbidity/mortality.
ECG pearls –
look for ST elevation in lead III greater than lead II or lead V1 (especially with ST depression in V2.
Right sided leads – elevation in V4R most specific but elevation in V3R-6R are indicative of RVMI. Keep V1 and V2
Give nitrates, which decrease preload, before diuretics. Diuretics are only indicated in volume overloaded patients, and many patient simply have fluid shifts and are overall euvolemic or have decreased plasma volume. Thus, in some patients, diuretics may be harmful.
Use non-invasive ventilation
BNP. The boards and ACEP recommend it but randomized clinical trials have not consistently demonstrated a benefit in the Emergency Department (Carpenter et al)
Right vs Left Sided Heart Failure – this distinction is someone artificial as chambers are interdependent in series.
Left-sided failure – pulmonary symptoms (dyspnea and orthopnea)
Right-sided failure have systemic venous congestion(pedal edema and hepatomegaly)
High Output Failure – conditions with excess cardiac output
Causes – increased preload (excess mineralocorticoids, fluid/salt retention), decreased systemic vascular resistance (pregnancy, cirrhosis, severe anemia, beriberi, thyrotoxicosis, Paget’s disease, or vasodilator medications), or tachycardia and persistent beta-adrenergic stimulation.
Treatment – correct underlying cause
Generously donated Rosh Review questions (scroll for answers)
Question 1. [polldaddy poll=8168396]
Question 2. A 73-year-old man presents to the ED with progressive shortness of breath for two days without chest pain. The patient has a history of hypertension controlled with hydrochlorothiazide, but has been noncompliant with his medications. In the ED, his vital signs are BP 186/102, HR 108, RR 34, and oxygen saturation 90% on room air. On exam, the patient has pulmonary crackles midway up both lung fields, jugular venous distension, and pitting edema of his lower extremities. A chest X-ray depicts increased interstitial markings and an enlarged cardiac silhouette. An ECG shows sinus tachycardia. [polldaddy poll=8168406]
Hollander JE, Diercks DB. Chapter 53: Acute Coronary Syndromes: Acute Myocardial Infarction and Unstable Angina.”Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011. p 367-385
Peacock WF. Chapter 57: Congestive Heart Failure and Acute Pulmonary Edema. Failure. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011 p 404-414
Answers:
Question 1. D. This patient presents with symptoms of acute decompensated heart failure (ADHF) and should be started on nitroglycerin therapy immediately. Patients with ADHF present with shortness of breath, increased work of breathing, tachycardia, hypoxia, crackles on lung examination and jugular venous distension. These patients experience acute worsening of left ventricular function and output secondary to a number of mechanisms including increased systemic vascular resistance. Therapy focuses on reduction of preload to decrease the flow of blood into the lungs and afterload reduction to increased the effectiveness of the left ventricle. Both of these goals can be accomplished through the administration of nitroglycerin. At lower doses, nitroglycerin acts as a peripheral vasodilator and increases venous capacitance leading to decreased preload. At higher doses, nitroglycerin causes arterial vasodilation leading to decreased afterload. Because of its rapid onset of action, nitroglycerin is the first line medication in patients with ADHF. Furosemide (A) may be useful in patients with volume overload and ADHF but this represents less than half of patients with ADHF. Additionally, the effects are delayed. Heparin (B) can be given in cases of ischemia induced ADHF but will not yield any immediate benefits. Morphine (C) was historically used as a preload reducer but has been associated with increased morbidity in patients with ADHF and is no longer recommended.
Question 2. A . This patient is in acute heart failure with pulmonary edema. The clinical presentation of heart failure includes shortness of breath, jugular venous distension, crackles and rales, peripheral edema, S3 gallop, orthopnea, and paroxysmal nocturnal dyspnea. A chest X-ray may show an enlarged cardiac silhouette, Kerley B lines suggesting pulmonary edema, and pulmonary vessel cephalization. Labs may show an elevated plasma brain natiuretic peptide (BNP). Management of heart failure with acute pulmonary edema begins with addressing the ABCs.Noninvasive respiratory therapy, such as bilevel positive airways pressure (BiPAP) or continuous positive pressure airway (CPAP) is the most appropriate next step in management. Noninvasive positive pressure ventilation increases oxygenation, decreases the worth of breathing, and decreases preload and afterload. In addition to BiPAP, adjunctive medications include nitrates, diuretics, morphine sulfate, and position the patient sitting up. Nitrates act as venous and arterial vasodilators and help to reduce preload and afterload. Morphine sulfate is thought to decrease oxygen consumption by decreasing catecholamines, decrease preload from mild vasodilator effects and decreases pain and anxiety. However, there are some studies that link the use of morphine sulfate to an increased mortality. Furosemide can be used in patients with evidence of fluid retention (JVD, extremity edema). Pulmonary edema secondary to heart failure usually responds well to preload and afterload reduction with noninvasive ventilation and nitroglycerin. If the patent continues to deteriorate then intubation (C) may be necessary. A myocardial infarction is less likely given the lack of chest pain and ECG that does not reveal ST-segment elevations. Therefore, activation of the cath lab (B) is unnecessary. Hydrochlorothiazide (D) has no role in the acute management of pulmonary edema. Once stabilized, the patient can resume his daily medications.
Question 3. Correct Answer ( C ) Atrioventricular (AV) conduction blocks occur in 25%–30% of patients with acute myocardial infarction. A narrow complex third-degree AV block in the setting of an inferior wall MI is usually transient and resolves spontaneously. Other AV blocks associated with a favorable prognosis include first-degree heart block and second-degree Mobitz type I (Wenckebach). Patients with a new left bundle branch block (A) in the setting of an acute MI are more likely to develop CHF, AV block, and ventricular fibrillation and have an overall increased mortality. Left posterior hemiblock (B) is associated with a large infarct size, increased risk of cardiogenic shock, and increased mortality. A new right bundle branch (D)in the setting of an anterior wall MI is associated with an increased risk of developing complete AV block and cardiogenic shock.
The Free Open Access Medical Education (FOAM) –from Dr. Ryan Radecki’s erudite blog, Emergency Medicine Literature of Note..
“Infections & Transfusions” – a JAMA meta-analysis found that higher hemoglobin targets were associated with an increased incidence of infection with a number needed to harm of 20-38. The group with a target level of 7-9 g/dL had an infection rate of 11.8% (95% CI, 7.0%-16.7%) compared with an infectious complication rate of 16.9% (95% CI, 8.9%-25.4%) in the “liberally” transfused group.
“Grilling Injuries on Memorial Day” – Grilling isn’t risk free. Dr. Radecki reviewed a case series of six individuals who presented in one year to a hospital after ingesting meat cooked on a grill. Three patients had neck pain with wire grill bristles removed via laryngoscopy and three had abdominal pain necessitating removal – 2 by colonoscopy and 1 with urgent surgery secondary to intestinal perforation.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapters 233; Rosen’s (8e) Chapter 7…but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
The Ones Our Patients Care About (Infectious – statistics are US based)
Bacterial contamination is rare: 1/500,000 – 1/1,000,000
Most common pathogen: Yersinia Entercolitica
More common in platelets: 1/1000-1/2000 per Rosen, CDC, and the AABB (Tintinalli cites 1 in 6 million)
Most Common virus: Parvovirus B19 (1 in 10,000). The others are very very rare: HIV and Hepatitis C > 1 in 1 million, Hepatitis B 1 in 100,000-200,000
Ingested Foreign Bodies
Beware the button battery. These can cause necrosis within hours in the esophagus and must be removed ASAP.
Objects that are irregular, very sharp, or have dimensions greater than 2.5cm in width or 6 cm in length that are still in the stomach or duodenum – call GI to have these removed via endoscopy.
Generously donated Rosh Review questions (scroll for answers)
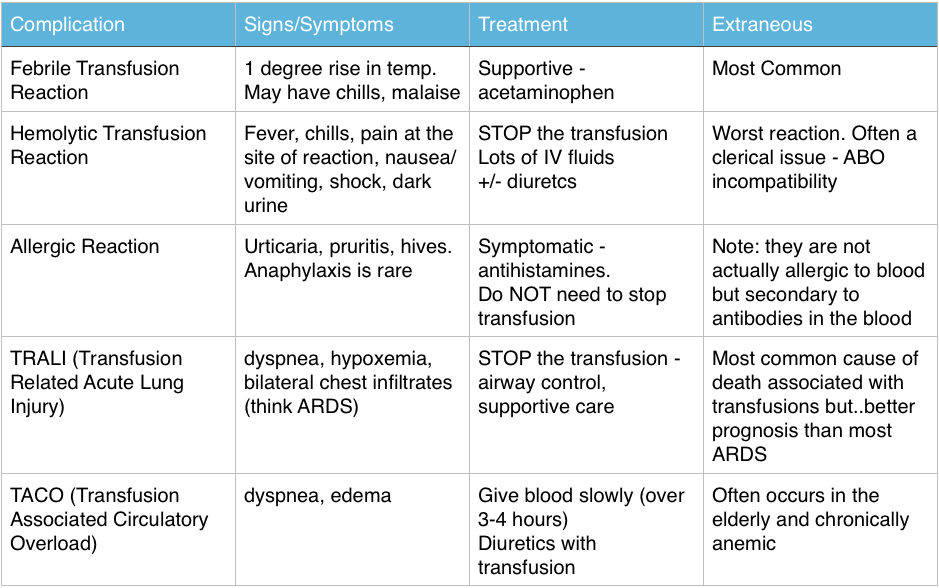
Question 1 A 55-year-old woman is receiving a blood transfusion due to persistent vaginal bleeding and a hemoglobin of 5 mg/dL. While receiving the transfusion, she develops fever, chills, back pain, pain at the site of transfusion, and tachycardia. [polldaddy poll=8109900]
Question 2 A 28-year-old man presents with a 1-day history of rectal bleeding. In the ED, he is hypotensive, thrombocytopenic, and is found to be passing melena. He receives a transfusion of platelets and packed red blood cells as part of his resuscitation. Twenty minutes after the start of his platelet transfusion, his BP is 90 mm Hg systolic, he becomes dyspneic, and his oxygen saturation drops from 99% on room air to 91% on 2L of oxygen supplementation. On exam, you note rales at the lung apices and that he is using accessory muscles to breathe. His chest radiograph shows diffuse interstitial infiltrates. [polldaddy poll=8109907]
Question 3 [polldaddy poll=8109908]
References:
Emery M. Blood and Blood Products. Rosen’s Emergency Medicine. 2014: 8th ed. p 75-80.e2
Coil CJ, Santen SA. Transfusion Therapy Tintinalli’s Emergency Medicine: A Comprehensive Review. 7th ed.
Hillyer CD, Josephson CD, Blajchman MA, et al. Bacterial contamination of blood components: risks, strategies, and regulation: joint ASH and AABB educational session in transfusion medicine. Hematology Am Soc Hematol Educ Program. 2003:575-89.
1. C – Up to 20% of all transfusions may lead to some type of adverse reaction. Although most of these reactions are minor, some are life-threatening. The patient is having an acute intravascular hemolytic reaction. This occurs when the recipient’s antibodies recognize and induce hemolysis of the donor’s red blood cells and may result in activation of the coagulation system and disseminated intravascular coagulation. This type of reaction typically presents with back pain, pain at the site of transfusion,headache, fever, hypotension, dyspnea, tachycardia, chills, bronchospasm, pulmonary edema, bleeding, and development of renal failure. First, stop the transfusion. Then initiate intravenous hydration to maintain diuresis.
2.D- This patient is most likely suffering from transfusion-related acute lung injury (TRALI), one of the leading causes of transfusion-related mortality. It is most closely associated with platelet and fresh frozen plasma transfusions, though cases have been reported with packed red blood cells since there is some residual plasma in the packed cells. Symptoms begin abruptly during transfusion or within 6 hours and resemble adult respiratory distress syndrome with noncardiogenic pulmonary edema, dyspnea, hypoxemia, and bilateral infiltrates on chest radiograph.
3. A- The patient is experiencing an allergic reaction without serious signs or symptoms. The transfusion does not need to be stopped for such a reaction; an antihistamine will help to relieve symptoms.