We are bringing you pearls from conferences we attend including SMACC (#smaccUS). This conference was amazing and we enjoyed meeting everyone. We look forward to seeing y’all at SMACC in Dublin June 13-16, 2016 and hope you check out the Free Open Access Medical education (FOAM) lectures from SMACC, in podcast form, until then.
Things in medicine aren’t always engineered to help us succeed. Engineering the environment smarter may make care safer. – Kevin Fong
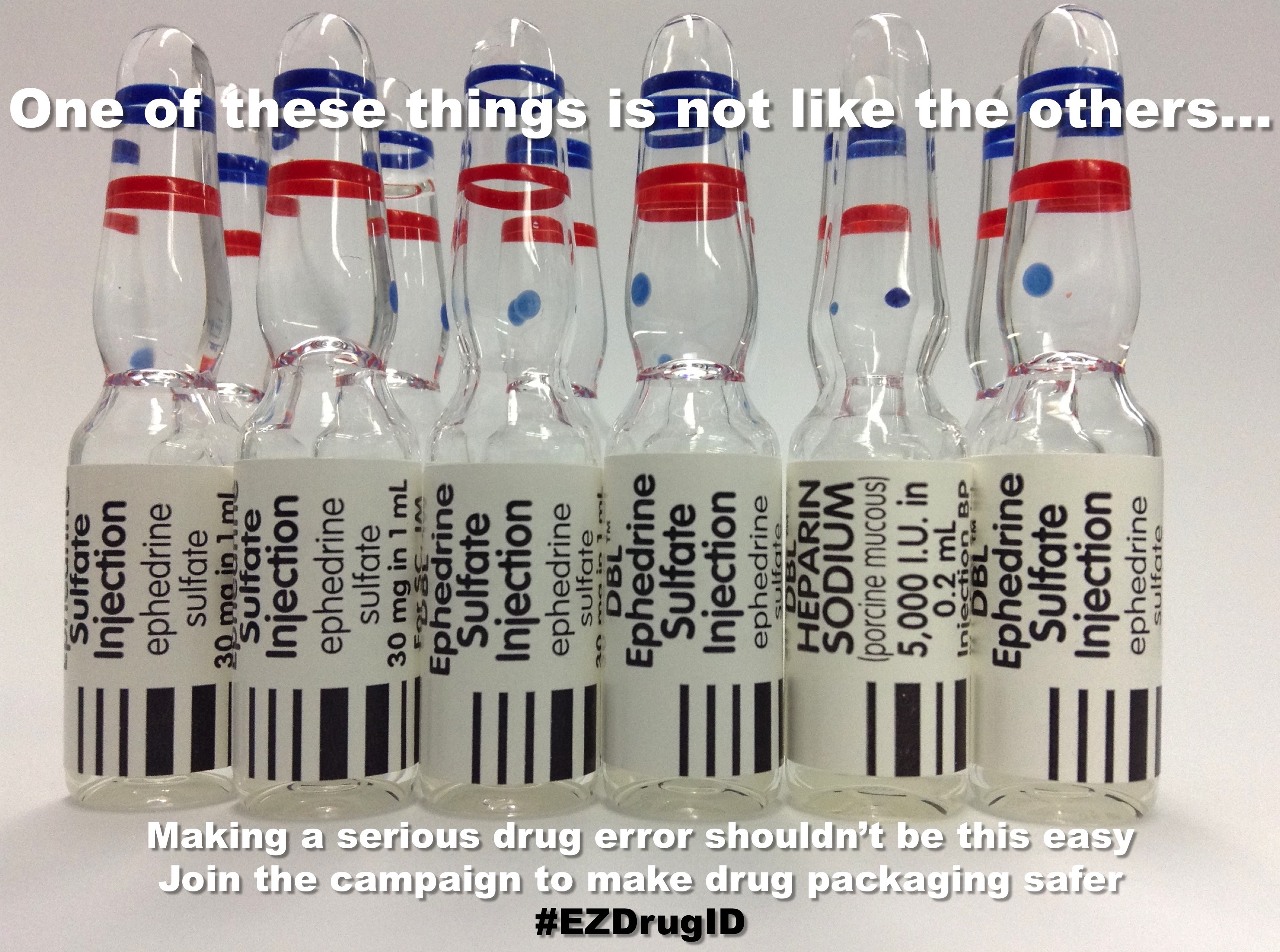
Medication vials often look quite similar and in a busy, heated moment this may lead to medication errors. Check out the EZdrugID project.
Photo: Dr. Nicholas Chrimes
Analgesia, there’s more to it than medicine – Jeremy Faust
Distraction is a good thing. Doing a painful procedure such as injecting local anesthetic? Distract the patient in tactile fashion by lightly scratching the patient proximal to the procedure. Alternative, music and videos can distract children and adults.
Calm music may reduce perception of pain.
Take advantage of child life, if you have them [AHRQ]!
The Glasgow Coma Scale is a problem – Mark Wilson (see this blog post)
The score doesn’t have intrinsic meaning. A GCS score can be associated with mortality ranging from 20-57%, depending on the individual components [Healey]
We’re really bad at assigning correct GCS scores to patients, even when we have cheat sheets [Feldman]
The interrater reliability of the GCS is abysmal [Bledsoe, Gill]
Describe the patient’s exam!
Shift work is disruptive – Haney Mallemat
Microsleep is dangerous, yet fairly common in the over tired provider
Replacing traditional night shifts with “casino shifts” may help. These are often comprised of 2 short shifts from 10p-4a and 4a-10a with the notion that each provider would get sleep during the “anchor period” of the Circadian cycle, 2am-6am. Small studies have shown this feasible, preferred by many, and perhaps perceived [Croskerry, Dukelow]
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The plenary, facilitated by the brilliant Dr. Victoria Brazil, focused on the impaired provider. At SMACC we’ve heard time and time again – we are fallible, we make mistakes.
Dying – Dr. Ashley Shreves
What often presume what our patients want without asking them. When dying patients are asked what they want, it comes down to dignity. 1) Being clean 2) Naming a decision maker and then other top priorities essentially come down to healthcare providers listening [Steinhauser et al]
We don’t ask patients about their code statuses appropriately. First, we often spend almost no time doing this. One study of hospitalists found that code status discussions lasted, on average, one minute. Further, that one minute was spent mostly focused on procedures [Anderson et al]
Communicate!
Evidence Based Medicine – The consensus of these cage matches was that evidence isn’t all equal; the existence of data doesn’t necessarily mean it’s good data.
The Randomized Control Trial (RCT) has problems – Drs. Paul Young and Simon Finfer
Caution with Base Rate Neglect – we jump to inappropriate conclusions. For example, pretend you have tested positive for a typically fatal disease. The test is accurate 95% of the time. Most people would conclude that there was a 95% chance they have the disease – a death sentence. Yet, one would need to know the prevalence of the disease in the general population to determine the actual likelihood that the test was correct. If the prevalence of the disease is 1 in 1000, the likelihood that you actually have the disease based on this test is <2%.
We should read the primary literature, but we can’t read all of it. Use FOAM (judiciously) – Drs. Rory Spiegel and Ken Milne
Due to the volume of literature, we have to make some decisions on what to read (Systematic reviews? Meta-analyses? RCTs? Case Reports?)
Severe traumatic brain injury can cause apnea which leads to a spiral of hypoxia (and thus cell death) and hypercapnea (with cerebral vasodilation causing cerebral edema) which can result in poor neurologic outcome.
The key? Resuscitate these patients as a hypoxic arrest. These are patients that need an airway and need oxygen.
We are bringing you pearls from conferences we attend including SMACC (#smaccUS). The overarching theme to Day 1 at SMACC? Use your team- to keep you in check and for feedback. Our cases and errors are opportunities for reflection. Dr. Cliff Reid reminded us to follow up our patients and outcomes and learn from it all, without letting our egos get in the way. Dr. Simon Carley (St. Emlyn’s) gave a powerful talk on learning from mistakes later in the day; you will definitely want to listen to these when they come out.
The sub theme? Experts don’t need algorithms and tests. But the novices? That’s another story.
Trauma – Weingart. We won’t delve into his thoughts on ATLS here (hint: ATLS isn’t for experts).
Ignore the first automated blood pressure, it’s probably wrong. Get a manual blood pressure.
Giving 3 units of blood in one hour? Prepare for massive transfusion, that means FFP, platelets, everything
If you go down the massive transfusion pathways, give an ampule of calcium every 4-6 units of plasma to combat the transfusion induced hypocalcemia from citrate.
The Shock Index (HR/SBP), isn’t as exciting as we once thought. It may be a guide, but not reliably so.
Pain – Strayer
Analgesia doesn’t = opiates. Think about local analgesia.
Pain as the “5th vital sign” – probably more harmful than helpful [Gussow]
In fact, in 2009, there were
Polypharmacy – Juurlink
Trimethoprim/sulfamethoxazole and ace-inhibitors/angiotensin receptor blockers, used in combination can lead to hyperkalemia and, in some cases, death [Juurlink et al]
Acetaminophen, at just 2 grams/day, can elevate the INR in patients on warfarin [Pinson]. Acetaminophen is still probably the analgesic of choice, but something to be aware of
Sepsis
Lactate is not a measure of tissue hypoxia/anaerobic metabolism [Marik et al]
Too much fluid is not a good thing = iatrogenic salt water drowning [Marik et al]
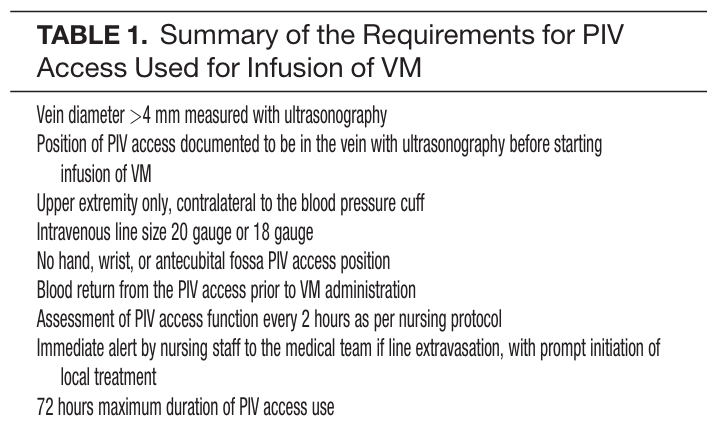
Patients may need vasopressors. If they do, don’t delay based on central access. Vasopressors are ok through good peripheral lines for a day or so. [Loubani et al, Mayo et al] However, we should probably place the lines when we’re safely able.
Of note, this does require strict protocols. Ex: Mayo study had stringent inclusion criteria
Thyroid disorders exist on a spectrum from myxedema coma to thyroid storm, with a large area in between.
Hyperthyroidism – too much thyroid hormones only from the thyroid gland
Thyrotoxicosis – too much thyroid hormone from any cause (i.e. taking too much thyroid supplement)
Thyroid Storm – see above. Thyrotoxicosis with increased adrenergic hyperactivity or abnormal response to the thyroid hormones by the peripheral tissues
Myxedema coma – These patients are the opposite of thyroid storm, all the systems are depressed (they are essentially hypo-everything). The diagnosis is clinical but these patients will have significantly elevated TSH with low T3/T4.
Altered mental status
Hypothermic, <35.5°C (95.9°F)
Hypotensive
Bradycardic
Hyponatremic
Hypoglycemic
Treatment –
Intravenous levothyroxine (T4) although endocrine may recommend that some patients get intravenous T3
Supportive care – passive rewarming, dextrose, intravenous fluids
1. A 28-year-old woman with no past medical history presents to the emergency department with acute dyspnea. Physical exam reveals tachycardia, warm extremities, wide-pulse pressure, bounding pulses, a systolic flow murmur, exophthalmos and a neck mass. [polldaddy poll=8935230]
2. [polldaddy poll=8936552]
Answers
1. This patient most likely has high-output heart failure secondary to thyrotoxicosis. High output heart failure occurs when cardiac output is elevated in patients with reduced systemic vascular resistance. Examples include thyrotoxicosis, anemia, pregnancy, beriberi and Paget’s disease. Patients with high output heart failure usually have normal pump function, but it is not adequate to meet the high metabolic demands. In high output heart failure the heart rate is typically elevated, the pulse is usually bounding and the pulse pressure wide. Pistol-shot sounds may be auscultated over the femoral arteries, which is referred to as Traube’s sign. Subungual capillary pulsations, often referred to as Quincke’s pulse, may be also be present. Although these findings may be seen in other cardiac conditions, such as aortic regurgitation or patent ductus arteriosus, in the absence of those conditions, these signs are highly suggestive of elevated left ventricular stroke volume due to a hyperdynamic state. Patients with chronic high output also may develop signs and symptoms classically associated with the more common low-output heart failure; specifically, they may develop pulmonary or systemic venous congestion or both, while maintaining the above normal cardiac output.
Low output heart failure (C) is often secondary to ischemic heart disease, hypertension, dilated cardiomyopathy, valvular and pericardial disease or arrhythmia. It can cause dyspnea but is not associated with symptoms of a hyperdyanmic state. Aortic regurgitation (A) is classically associated with bounding pulses, a wide pulse pressure and subungual capillary pulsations; however, aortic regurgitation is less likely in a young woman with no past cardiac history. Additionally, this woman has exophthalmos and a goiter on exam, which support the diagnosis of thyrotoxicosis. Methamphetamine intoxication (D) usually presents with agitation, tachycardia, and psychosis; however, it is not associated with a hyperdynamic state, exophthalmos or a goiter.
2. Hyperthyroidism is a condition in which there is overproduction and increased circulation of thyroid hormone. Hyperthyroidism has a variety of causes and variable presentation. Increased circulating thyroid hormone causes a hypermetabolic state and increases beta-adrenergic activity. Initially, patients may have vague constitutional symptoms. As the disease progresses, clinical manifestations may become more organ-specific. Thyrotoxicosis or thyroid storm represents the most severe manifestation of the disease. Thyroid storm is life threatening and characterized by hyperadrenergic activity. Patients present with vital sign abnormalities including tachypnea, tachycardia, hyperthermia and hypertension. ECG may show atrial dysrhythmias like atrial flutter and fibrillation or simple sinus tachycardia. High-output cardiac failure is common as well. Physical features include goiter, opthalmopathy and tremors. Patients will also have increased reflexes and altered mental status. Thyroid storm treatment involves suppression of thyroid hormone synthesis and secretion, prevention of peripheral conversion from T4 to T3 and blocking the peripheral adrenergic stimulation. Blocking the peripheral effects of thyroid hormone is best accomplished with a beta-blocker and propranolol is preferred as it also decreases conversion of T4 to T3.
Lithium (A) is a cause of hypothyroidism. In hyperthyroidism, TSH is depressed (C). Weight gain (D) is common in hypothyroidism.
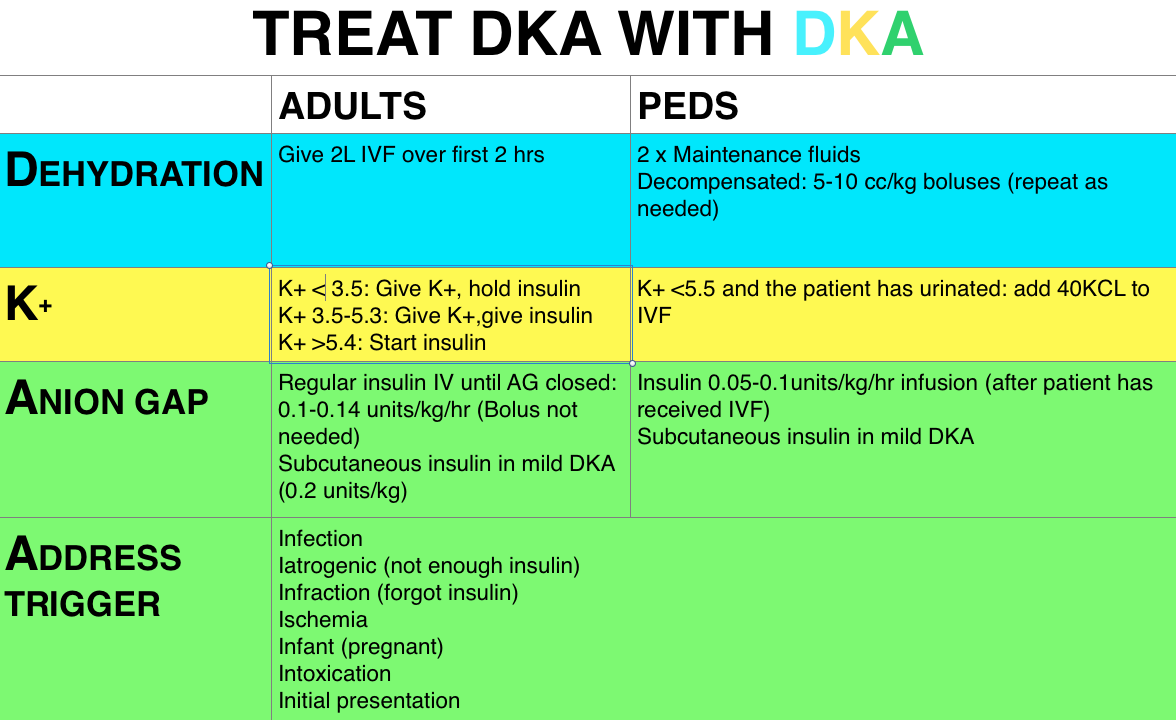
Fluids come first in DKA but you may not need as much as you think. They recommend only using fluid boluses, and even then a baby bolus of 5-10 cc/kg, in the hypotensive decompensated patients, coupled with frequent re-assessments. Other patients can get up to twice maintenance of 0.9% NaCl.
No insulin bolus for pediatric patients, ever.
Cerebral edema is the most dreaded complication of DKA and seems to be associated with severe presentations, young children (<5), or DKA as the presentation of diabetes. Treatment related factors such as administration of an insulin bolus or sodium bicarbonate may also contribute. The role of fluids (particularly over-aggressive fluids) is less clear [1-3].
Management of cerebral edema: ABCs, Elevate head of the bed 30 degrees, Mannitol 0.5-1g/kg IV over 20min AND/OR hypertonic (3%) NaCl 5-10cc/kg IV over 30min
The Bread and Butter
We cover hyperglycemia including diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS). We do this based on osen’s Emergency Medicine, Chapter 126 (8th ed) and Tintinalli, Chapter 222 (7th ed). But, don’t just take our word for it. Go enrich your fundamental understanding yourself.
Workup – evaluate electrolytes (particularly potassium) and potential triggers for DKA.
Treatment – fluid resuscitation is initial intervention as these patients are typically 4-6 L down. In adults we hold insulin treatment until we know the patient’s serum potassium, as these patient’s are depleted secondary to osmotic diuresis. Further, the patient’s serum potassium may be falsely elevated by acidosis. Insulin may be started once the potassium is >3.5 (with potassium replacement if <5.3). We do not bolus pediatric patients but the ADA guidelines and Rosenalli state we do not need the insulin bolus in adults either [4-6]. The use of subcutaneous insulin in DKA is popular amongst pediatric patients and growing in popularity in adults [7,8].
Hyperosmolar Hyperglycemic State (HHS)
Diagnosis – elevated serum glucose (often >600 mg/dL), serum osmolar >315-320 mOsm/kg. Patient’s may have a concomitant acidosis or ketosis, but this is often less profound than in DKA.
Workup – ascertain why the patient ended up in HHS – whether it was a mobility issue or polypharmacy (diuretic, lithium, etc). Check osmolality and for DKA.
Treatment – these patients are often severely dehydrated (>8 Liters). Start with volume resuscitation and add an insulin infusion (0.1 units/kg/hr).
1. A 43-year-old man presents with altered mental status. His vital signs are HR 113, BP 143/63, T 98.9°F and blood glucose of 750 mg/dl. During your evaluation he has a brief generalized tonic-clonic seizure. [polldaddy poll=8904849]
Answers
1. This patient presents with signs and symptoms consistent with hyperglycemic hyperosmolar state (HHS) and intravenous fluids should be given aggressively early in management. HHS is a syndrome characterized by dehydration, hyperglycemia, hyperosmolarity and altered mental status. Patients may present with confusion, lethargy, seizures, focal neurologic deficits or frank coma. Pathophysiologically, decreased insulin (or insulin action) leads to gluconeogenesis and increased circulating glucose levels. This in turn draws fluid from the intracellular space into the intravascular space. The resultant osmotic diuresis leads to profound intravascular dehydration, electrolyte abnormalities and hyperosmolarity. Typically, patients will have a blood glucose >600 mg/dl and an osmolarity >350 mOsm/L. Blood urea nitrogen and creatinine are usually elevated. Initial management focuses on supportive care and aggressive fluid resuscitation. Patients with HHS are estimated to be 5-10 liters behind. In addition to fluid administration, electrolyte repletion is paramount.
2. A 45-year-old man presents with altered mental status. On arrival, his finger stick is 35 mg/dL. He is given dextrose leading to the return of a normal mental status. On history, he reports he may have accidentally taken extra medication. Which of the following medications requires prolonged observation in the hospital?
Glipizide
Metformin
Novolog
Sitagliptin
In most adults, symptomatic hypoglycemia occurs when glucose levels reach 40 to 50 mg/dL. Glipizide is a sulfonyurea oral hypoglycemic drug. This class of medication is associated with hypoglycemic episodes through their action as an insulin secretagogue. In a sulfonylurea overdose, patients should be observed for 24 hours. When the etiology is unclear, laboratory testing including renal function is indicated. In situations without large ingestions, patients may be discharged if no additional episodes of hypoglycemia occur after an observation period. In cases of severe, prolonged or recurrent episodes of hypoglycemia from sulfonylureas, additional therapy with octreotide as an inhibitor of insulin release is indicated.
References:
Glaser NS, Wootton-Gorges SL, Buonocore MH, et al. Subclinical cerebral edema in children with diabetic ketoacidosis randomized to 2 different rehydration protocols. Pediatrics. 2013;131(1):e73–80. doi:10.1542/peds.2012-1049.
Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. N Engl J Med. 2001;344(4):264–9. doi:10.1056/NEJM200101253440404.
Lawrence SE, Cummings E a, Gaboury I, Daneman D. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. J Pediatr. 2005;146(5):688–92. doi:10.1016/j.jpeds.2004.12.041.
Diabetic Emergencies : New Strategies For An Old Disease.
Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–43. doi:10.2337/dc09-9032.
Goyal N, Miller JB, Sankey SS, Mossallam U. Utility of initial bolus insulin in the treatment of diabetic ketoacidosis. J Emerg Med. 2010;38(4):422–7. doi:10.1016/j.jemermed.2007.11.033.
Umpierrez GE, Cuervo R, Karabell A, Latif K, Freire AX, Kitabchi AE. Treatment of diabetic ketoacidosis with subcutaneous insulin aspart. Diabetes Care. 2004;27(8):1873–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15277410. Accessed July 17, 2014.
Umpierrez GE, Latif K, Stoever J, et al. Efficacy of subcutaneous insulin lispro versus continuous intravenous regular insulin for the treatment of patients with diabetic ketoacidosis. Am J Med. 2004;117(5):291–6. doi:10.1016/j.amjmed.2004.05.010.
We enjoy contributing to the Free Open Access Medical education (FOAM) community. Creating FOAM is not free and requires significant costs in time and money. Yet, we find this investment invaluable and appreciate everyone who listens, as well as those who champion our endeavor (including the supportive people in our life that tolerate “FOAMcast dates” and tiptoe around whilst recording). We would also like to thank everyone who has contributed by means of post-publication peer review (Brett Schupack, Dr. Marc Probst, Dr. Gabriel Cade, Dr. Iain Beardsell, and countless others). Please continue to not only let us know when we get it right, but also when we get it wrong. We appreciate the suggestions, praise, feedback, and corrections.
Given our love of spaced repetition, we review our favorite pearls and mnemonics from the past year.
HANG IV: hernia, adhesions, neoplasm, gallstone (ileus), intussception,
Heart failure episode – treatment for right ventricular heart failure.
Optimize OHCRAP – Oxygenation, Hemodynamics, Contractility, Rate/rhythm, Afterload, and Preload
Headaches – Likelihood of migraine diagnosis (comes from the outpatient literature) = POUND. 4 criteria very indicative of migraine (+LR 24), 3 criteria also likely (+LR 3)
Pounding headache
hOurs: headache lasts 4-72 h without medication
Unilateral headaches
Nausea
Disabling: disrupts daily activities
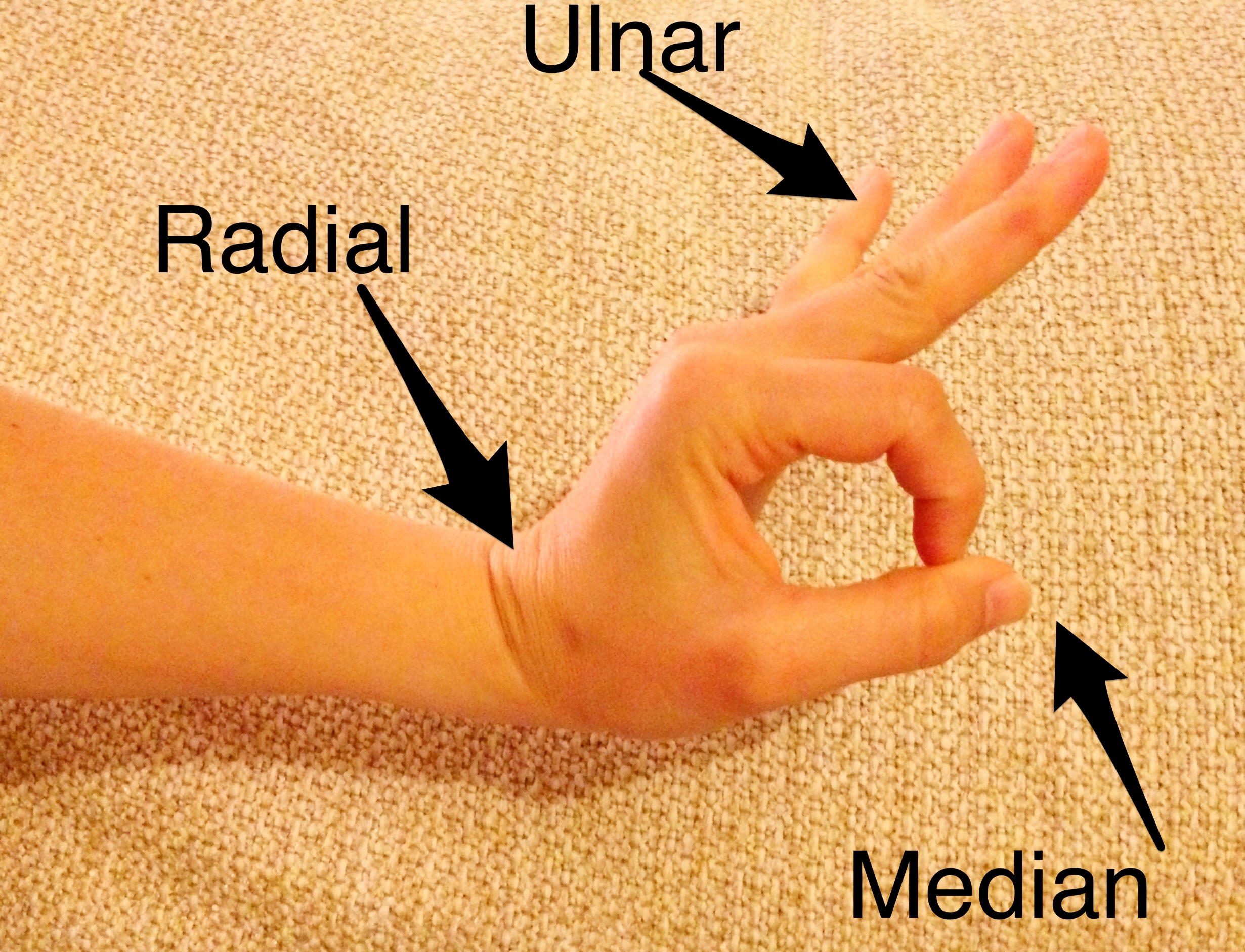
Our most frequently used clinical pearl:
The hand exam, in one movement:
Motor Exam of the Hand
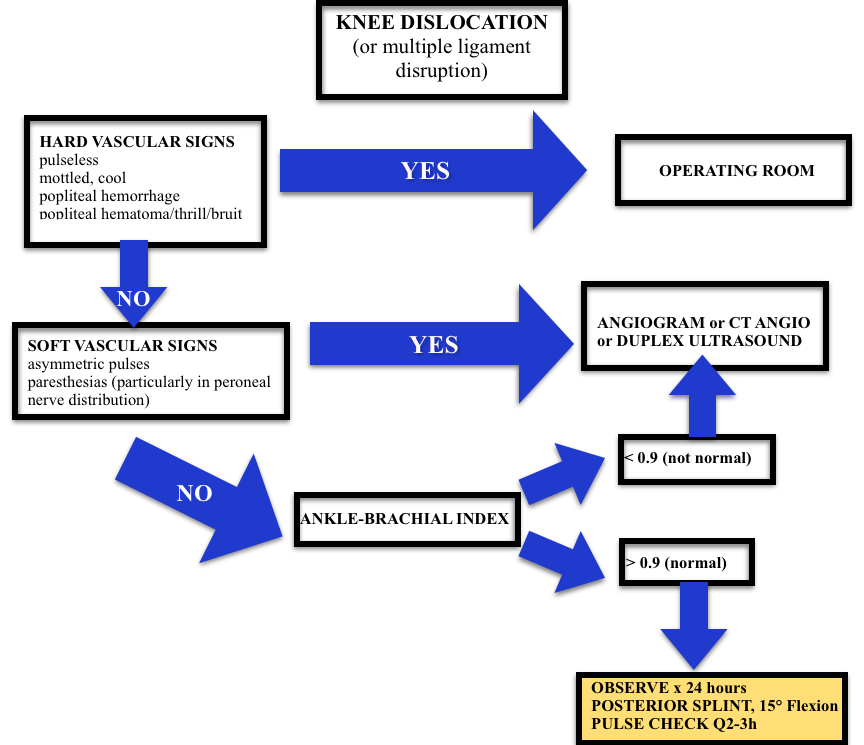
Our favorite visual aid:
Burns – Grading the burn according to the Egyptian flag (because we all knew what that looked like).
Burn Degree
Worst visual aid: the Knee volcano (we won’t go there again)
Cord – complete cord syndrome that persists longer than 24 hours is highly unlikely to have any motor recovery. These patients need urgent intervention. This is we must differentiate between the complete and incomplete cord syndromes. Complete = “total loss of motor power and sensation distal to the site of the spinal injury.”
Knee/Leg– Beware knee dislocations. Of patients with popliteal disruption, the amputation rate rises to 90% 8 hours after the injury without surgical intervention.
Knee Dislocation Algorithm
Time is skin?
Hey Jeremy, re burns – surely needed a ‘Time is skin’?? @FOAMpodcast
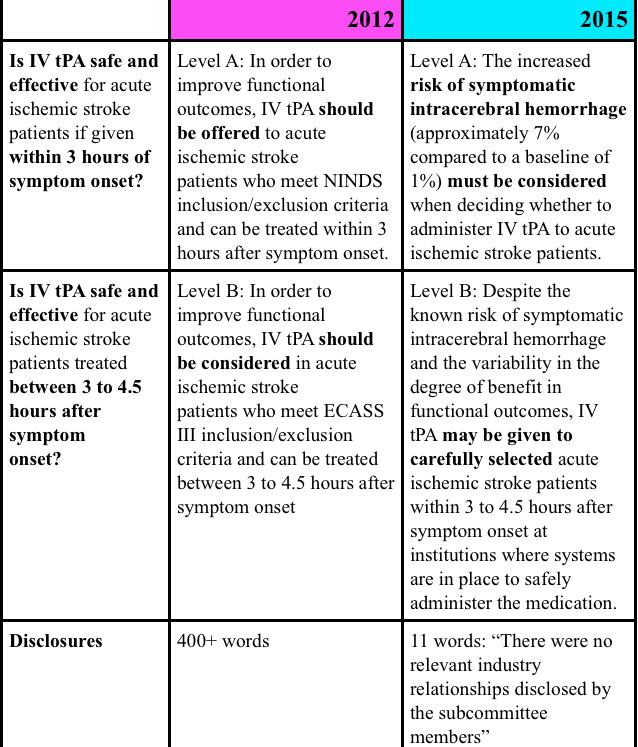
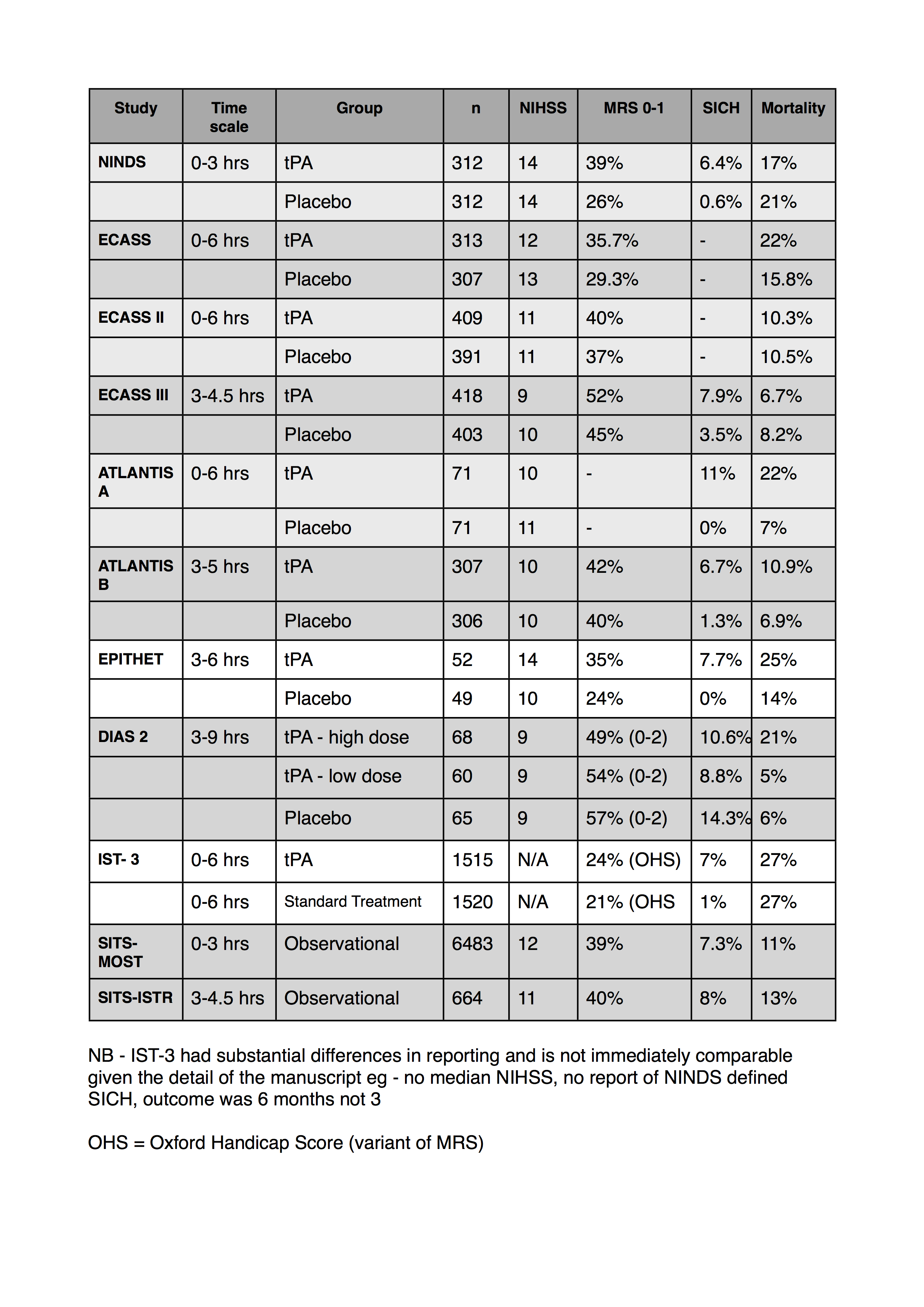
ACEP tPA Clinical Policy 2012 – This policy has been entrenched in controversy since it was published. Why? Well, largely because the evidence was given a stronger level recommendation than the data supported, conflicts of interest abounded, and the data (mostly from NINDS (The SGEM review), ECASS, and IST-3) were problematic. This has been well covered by these reviews of the clinical policy:
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. Weekend review, Monday review, Tuesday review
Scientific Assembly Wednesday Pearls
(there’s too much to choose from, so follow #ACEP14)
Debating Clinical Policies: Implications for tPA and Beyond – Drs. David Newman, David Seaberg, and Edward Sloan
The ACEP clinical policy on TPA is hotly debated, as it gives Level A evidence to TPA in acute ischemic stroke. This policy is being reconsidered and big props to ACEP for doing this, most professional organizations aren’t that responsive.
TPA has a NNT of 8 and a NNH of 16. The TPA supporters typically reference NINDS, ignoring the other RCTs. They also reference large sets of registry data.
Evidence-Based Approach to the “Other” Stroke – Dr. Jon Edlow
Prothrombin complex concentrate (PCCs) are all the rage, particularly since the 4 factor PCC was approved last year in the United States. It improves patients numbers of coagulopathy, but not necessarily patient outcomes (Dr. Rory Spiegel on the topic).
Fresh frozen plasma, dosing is based on INR and the patient’s weight, it’s not an empiric “2 units.”
Blood pressure control may be safe in Intracerebral hemorrhage, but the studies such as INTERACT don’t show that it benefits patients (The SGEM).
Chest Pain in the ED: Is One Troponin Enough? – Dr. David Newman
The miss rate for MI is often quoted as 2%, but it’s more like 0.2% per the Pope et al study. So, we’re pretty good at this.
ACEP has a policy stating that a single troponin after 8 hours of chest pain is sufficient
States that have tort reform have shown fewer lawsuits and less money without compromising patient outcomes.
Clinical Pearls From the Recent Medical Literature – Drs. Jerome Hoffman and Richard Bukata (#hofkata)
Topical analgesia for corneal abrasions – the FOAM world has been buzzing with the notion of using tetracaine for corneal abrasions (Rebel EM, The SGEM). Hofkata reviewed this paper by Waldman et al that showed no difference in visual analog scores for normal saline compared with tetracaine for corneal abrasions. Tetracaine was perceived more effective so there may be a role for dilute proparacaine but we’ll need some more studies.
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. Weekend review, Day 1 review.
Scientific Assembly Day 2 Pearls
(there’s too much to choose from, so follow #ACEP14)
Simple Complaints in Patients with HIV – Dr. John Perkins
HIV is a risk factor for coronary artery disease (CAD) and these patients are prone to thrombotic complications [Boccara et al]
Dr. Amal Mattu has really championed this point, as in this videocast
Resuscitation Pearls – Dr. Scott Weingart
REBOA and ECMO are exciting and coming…but most of us don’t have them. Watch the literature.
“Normal” vital signs shouldn’t reassure us in trauma. Don’t wait for patients to become hypotensive (this is a danger of euboxia)
The Shock Index (Heart Rate/Systolic Blood Pressure) is one way to help detect badness amongst “normal” vital signs in these patients (See this post)
ACLS algorithms, they’re helpful for people who don’t specialize in resuscitation. Think about the individual patient and target interventions accordingly. Oh, and do good CPR.
The AHA supports this, for example, they recommend against the routine use of calcium and sodium bicarbonate [2010 Guidelines].
End of Life/Palliative Care – Dr. James Adams
Hospice and palliative care are INTENSIVE. Listen to Dr. Ashley Shreves on the EMCrit podcast if you’re not convinced of this (actually, listen regardless, it’s worth it).
A Do Not Resuscitate (DNR) order only speaks to whether or not a patient wants CPR if they die. No more, no less. But, for more on this, check out this blog post.
In general, physicians don’t broach end-of-life topics with patients. Dr. Adams quoted a statistic “Approximately 50% of doctors don’t know their patient’s resuscitation wishes.” The consensus in the room was that it really doesn’t take that much time to initiate these conversations but brief questions asking about a patient’s wishes, checking in to see if they have sufficient resources, or. (Lauren’s take on the topic).
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. However, Jeremy and I both worked overnights so we got into town a little late. Our friends and ACEP luminaries, Drs. Justin Hensley, Howie Mell, and Todd Slesinger.
Naloxone (Narcan) – The council approved resolutions in support of naloxone for everyone. There was also a resolution on developing a clinical policy for emergency physicians prescriptions of naloxone. Watch out for it.
Medical Marijuana – Apparently http://www.mindanews.com/buy-inderal/ every year brings some bickering about medical marijuana….and every year, the council defeats the resolutions. This year was no different…no support for medical marijuana from ACEP.
Emergency Department Pharmacists – These folks are indispensable in the ED (and in the FOAM world), and ACEP recognized this with the passing of Resolution 44 (what this means, clinically, not sure). And if you haven’t work with them – you’re missing out. We’re huge fans of EMPharmD and, naturally, Bryan Hayes (@PharmERToxGuy)
There’s also a lot of politics that goes into these bills, for that part, we got Dr. Kevin Klauer, Council Speaker on FOAMcast to explain.
But the real news… Dr. Kevin Klauer’s haircut.
Dr. Kevin Klauer’s former look
Wow, Klauer got a haircut. Amazing. Still the same brain, just no bangs flip… pic.twitter.com/hmYtKKQyHc