FOAMcast brings you pearls from conferences we attend and presently it’s the American College of Emergency Physicians annual meeting, ACEP15 in Boston. On this episode we cover the following topics:
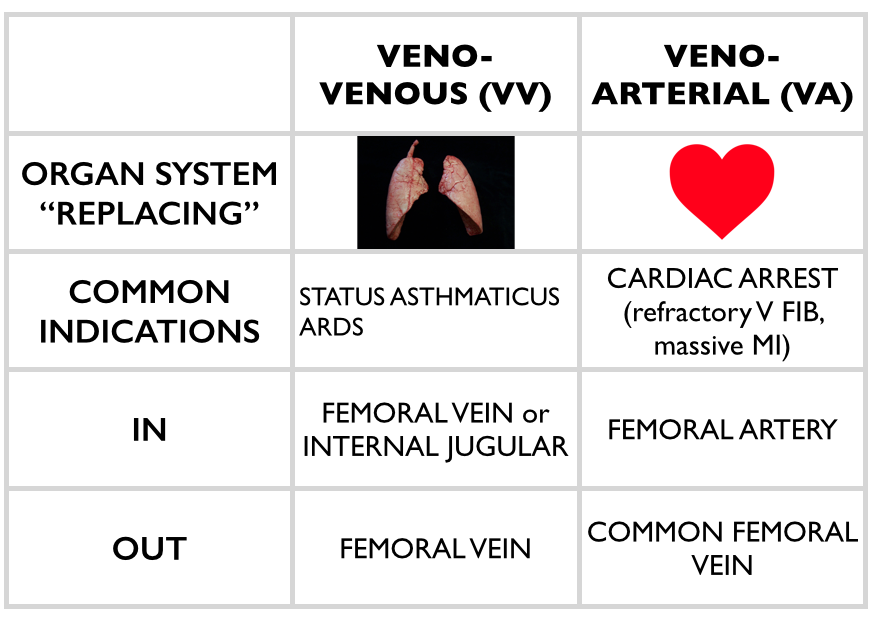
Extracorporeal Membrane Oxygenation (ECMO) – Dr. Haney Mallemat (@CriticalCareNow)
ECMO is promising in certain devestating disease processes – essentially heart or lung failure. For example, in the CHEER trial, the investigators had a 54% rate of neuro-intact survival after cardiac arrest with ECMO []. Yet, ECMO can be confusing. Dr. Mallemat simplified this for the emergency physician (see this site for more complete explanations)
Stop the Madness: Diagnostic Imaging in Nephrolithiasis – Workshop with Drs. Eddy Lang, Rebecca Smith-Bindman, Grant Innes, and Lauren Westafer
FOAMcast brings you pearls from conferences we attend and presently it’s the American College of Emergency Physicians annual meeting, ACEP15 in Boston.
Jeremy Hoffman and Rick Bukata summarize recent, relevant literature each year (recently known as #hofkata). This year, our top three favorite
Dr. Jeff Kline (@klinelab) spoke on pulmonary embolism.
High Risk PE? Consider lysis (this is controversial, we are simply reporting Dr. Kline’s talk)
Size and location. Massive and proximal= bad
SBP <90 for more than 15 min OR 40mmHg drop from baseline
Signs of RV strain – echocardiography showing RV dilation OR hypokinesis?
Elevated troponin or BNP
ECG findings suggestive of cardiac strain: sinus tachycardia, incomplete right bundle branch block, complete right bundle branch block, T-wave inversion in leads V1 – V4.
Kline also participated in a knowledge translation workshop where he argued that sub-segmental PEs, without DVT on ultrasound, are NOT a real thing. This is controversial but he also argued that treating these is associated with harm [Carrier et al]
Chest x-ray initial test of choice – may miss 50% of fractures, unclear if this is clinically significant [6]
Ultrasound has found to have excellent sensitivity [7]
Rib films are NOT recommended [4-6].
Complications: Traumatic rib fractures may be associated with other traumatic injuries such as pneumothorax, hemothorax, or in the case of lower rib fractures, intra-abdominal injury. However, rib fractures themselves have been associated with mortality, most often as sequelae of pulmonary embarrassment including pneumonia, intubation, and death. Mortality in elderly patients with rib fractures is significantly higher than the younger counterparts at 22% and 10% respectively [8,9].
Mortality is between 3-13%
Risk stratification (see this post): Battle and colleagues developed a prognostic scoring system, not externally validated and unclear if it would change practice, that highlights common sense predictors of poorer outcomes:
Age (>65)
Higher number of rib fractures
Chronic lung disease
Hypoxia (<90%)
Pre-injury anticoagulant use [11]
Treatment
Analgesia:
Often includes NSAIDS (ibuprofen), acetaminophen, and narcotics +/- gabapentin (ibuprofen and gabapentin depending on renal function)
Epidural analgesia – highly recommended in the EAST guidelines [14].
Paracostal analgesia (ex: ON-Q pump) – not sufficient evidence for EAST recommendation (2005) [14]
Pulmonary Hygiene (formerly pulmonary toilet): involved incentive spirometry, coughing, mobilization (up, out of bed), and possibly chest physical therapy
ORIF, “rib fixation” or “rib plating,” is increasingly common in the US and studies have found improvements in ICU LOS and ventilator days [15]
Disposition
Many rib fracture patients will need to be admitted to the hospital for pain control, observation, and pulmonary hygiene.
Some rib fracture patients may benefit from care at trauma centers. Lee et al wrote that 3+ rib fractures exists as an indication for transfer to a level 1 trauma center and many places ascribe to this, it depends on the hospital and physicians.
While patients in the ED may look good, patients may benefit from high intensity floors (ie stepdown units) and many patients get observed in ICUs, again, depending on local practice patterns. Some protocols risk stratify patients (i.e. to the ICU vs floor) by incentive spirometry.
Patients with adequate pain control who are low risk (younger, <3 rib fractures, good effort on incentive spirometry) may be discharged from the ED with analgesia and education on importance of pulmonary hygiene
Sternal Fractures – more common with ubiquity of airbags and seatbelts.
Diagnosis: Classically the “gold standard” has been lateral x-ray. However, CT technology has improved since those studies. Ample literature suggests that ultrasound has excellent sensitivity [1-3].
Complications: Historically, sternal fractures were associated with injuries of the great vessels, high mortality, and blunt cardiac injury (BCI) [16-18]. The most recent iteration of the EAST guidelines states, “the presence of a sternal fracture alone does not predict the presence of BCI and thus should not prompt monitoring in the setting of normal ECG result and troponin I level” (Level 2) [18].
Treatment: Analgesia. Most patients with isolated sternal fractures (no pneumothorax, hemothorax, BCI, or hemodynamic instability) that have adequate pain control can be discharged from the ED [1-2].
Blunt Cardiac Injury
A broad category including a range of injuries from clinically silent dysrhythmias to cardiac wall rupture or vasospasm. BCI often results from high impact injury and should be considered in patients with significant thoracic trauma including rib fractures, sternal fracture, pneumothorax, hemothorax, and pulmonary contusion.
Diagnosis: There is no gold standard test. One can rule out BCI with a normal ECG and a single normal troponin I [18].
Management: If an ECG or troponin is abnormal, admit to telemetry for monitoring and echo.
Question 1. A 23-year-old man presents with chest pain after a motor vehicle collision. The patient’s chest struck the steering wheel. He has no other complaints or injuries. Chest X-ray is unremarkable. ECG shows sinus tachycardia with anterior ST depressions. A troponin is sent and is positive at 3.50 mg/dl. [polldaddy poll=9134639]
Question 2. A 20-year-old man presents with left rib pain after falling while playing soccer and striking his chest. Vital signs are normal. On physical examination, the patient has tenderness to palpation over the 4th rib in the midaxillary line. [polldaddy poll=9134640]
Question 3. A 32-year-old woman was the restrained driver involved in a head-on motor vehicle collision (MVC) 2 days prior to presentation. She is complaining of chest pain and bruising to her chest. Her blood pressure is 118/78 mm Hg, pulse is 88 beats/minute, respirations are 18 breaths/minute and oxygen saturation is 96% on room air. You note bony tenderness and ecchymosis to her sternum. You order a chest X-ray and diagnose a non-displaced sternal fracture. [polldaddy poll=9134643]
Answers
This patient presents with a myocardial contusion and should have an echocardiogram performed to look for any cardiac damage. Myocardial contusion describes a nebulous condition. It can occur through several mechanisms including a direct blow to the chest and compressive force over a prolonged period of time. Histologically, the disorder has similar findings to those seen after acute myocardial infarction. The majority of contusions heal spontaneously but small pericardial effusions may develop. Delayed rupture after resorption of hematoma is feared but rare complication. Patients with myocardial contusion will present after trauma with external signs of trauma and typically have other concomitant thoracic lesions (pulmonary contusion, pneumothorax, hemothorax). Patients will typically have tachycardia (up to 70%). ECG may show dysrrhythmia or ST changes but may also be normal. Although it is not effective to admit all patients for workup for myocardial contusion and the disease has a very low rate of cardiac complications, in the presence of ECG changes and elevated biomarkers, observation and echocardiography are a reasonable approach. Echocardiogram can be used to diagnose pericardial effusion, thrombi formation and valvular disruption.Cardiac catheterization (A) is not necessary after a myocardial contusion as coronary artery obstruction is not part of the pathophsyiology. The patient should not be discharged home (B)without an echocardiogram. Pericardiocentesis (D) is only necessary in the presence of a large pericardial effusion or one causing cardiac tamponade.
This patient presents with signs and symptoms consistent with a rib facture. A chest X-ray should be performed to rule out any other pathology including pneumothorax and pulmonary contusion. Rib fractures are a common injury after thoracic trauma and the incidence increases with increasing age. They may be associated with a number of potential complications including pulmonary contusions, hemothorax, penumothorax and post-traumatic pneumonia. Fractures are most common at the posterior angle, which represents the weakest area. The ribs most commonly fractured are the 4th – 9th ribs. The 9th – 11th ribs are mobile, which reduces the risk of fracture. However, fractures of these ribs are more likely to be associated with intraabdominal injuries. Rib fractures should be suspected based on history and clinical evaluation. Patients will present with chest pain and tenderness over the area. Imaging should be obtained to rule out the more serious associated complications of pneumothorax, hemothorax and pulmonary contusion. Chest X-ray is the appropriate modality for this but often will not demonstrate the presence of a single rib fracture when it is in fact present. This is particularly true of non-displaced fractures. Rib belts (B) are discouraged as they may decrease the depth of respiration and lead to atelectasis and pneumonia. CT scan of the chest (D) is not routinely required for management of a simple rib fracture. Analgesia and discharge home (A) is likley to occur once more serious pathology is ruled out with a chest X-ray. Patients with rib fractures should also receive an incentive spirometer to help reduce the complication of pneumonia.
Isolated, non-displaced sternal fractures are associated with low overall mortality rates. Fractures and dislocations of the sternum are caused primarily by anterior blunt chest wall trauma during a head-on MVC. Isolated fractures of the sternum most commonly occur when the chest wall is thrust against a diagonal seatbelt strap during rapid deceleration in a frontal impact MVC. They are more common in older individuals and women. Most fractures are transverse and non-displaced and can be diagnosed on a lateral chest radiograph. Although a fracture of the sternum can be seen following major thoracic trauma, its presence alone does not indicate severe underlying thoracic injury. However, if other significant underlying thoracic injuries are suspected, a CT-scan of the thorax should be performed
References:
You JS, Chung YE, Kim D, Park S, Chung SP. Role of sonography in the emergency room to diagnose sternal fractures. Journal of clinical ultrasound : JCU. 38(3):135-7. 2010. [pubmed]
Engin G, Yekeler E, Güloğlu R, Acunaş B, Acunaş G. US versus conventional radiography in the diagnosis of sternal fractures. Acta radiologica (Stockholm, Sweden : 1987). 41(3):296-9. 2000. [pubmed]
Jin W, Yang DM, Kim HC, Ryu KN. Diagnostic values of sonography for assessment of sternal fractures compared with conventional radiography and bone scans. J Ultrasound Med. 2006 Oct. 25(10):1263-8; quiz 1269-70.
”Pulmonary Trauma” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. Ch 258.
Livingston DH, Shogan B, John P, Lavery RF. CT diagnosis of Rib fractures and the prediction of acute respiratory failure. The Journal of trauma. 64(4):905-11. 2008. [pubmed]
Karangelis D, Koufakis T, Spiliopoulos K, Tsilimingas N, Bouliaris K, Desimonas N. Management of isolated sternal fractures using a practical algorithm. J Emerg Trauma Shock. 7(3):170-. 2014. [article]
Dua A, McMaster J, Desai PJ et al. The Association between Blunt Cardiac Injury and Isolated Sternal Fracture. Cardiology Research and Practice. 2014:1-3. 2014. [article]
This is an exciting week of primary literature, particularly as many large critical care trials were published in major journals despite being “negative studies.” We are excited by this as, too often, we see “negative studies” discarded. Further, these studies examined things some practices we seem to believe in: balanced crystalloids, apneic oxygenation (see Dr. Scott Weingart’s podcast on the FELLOW study), treating fever. We love that the Free Open Access Medical Education (FOAM) community and study authors are examining beloved practice and open to questioning the very things we believe in. Well done.
We cover two core content papers out by Dr. Paul Young (@dogICUma) in JAMA and NEJM this week. His trials are as clever as his Twitter handle.
SPLIT – The FOAM world has sung the praises of balanced fluids given they have more physiologic composition. The thought, as detailed in this post, is that 0.9% NaCl contains an ABnormally large amount of chloride which may cause a hyperchloremic metabolic acidosis. Prior literature suggests an increased incidence of kidney injury with saline compared with balanced solutions. Thus, Dr. Paul Young and colleagues sought to study this with the best trial, to date, on this topic.
Multicenter, blinded, cluster-randomized, double-crossover trial of adult ICU patients receiving crystalloids randomizing patients to 0.9%NaCl or Plasma-lyte (balanced solution).
Sites used one fluid for seven weeks and then crossed over to the other fluid (labeled Fluids A and B).
Primary outcome: AKI according to the RIFLE criteria within 90 days – no difference between groups.
9.6% in Plasma-lyte group vs 9.2% in the saline group (absolute difference 0.4% [95% CI, −2.1%-2.9%]; RR, 1.04 [95% CI, 0.80-1.36]; P = .77)
Secondary outcomes: No difference in renal replacement therapy, ICU days, mechanical ventilation, or mortality
A few things to keep in mind:
70% of patients were admitted to the ICU from the OR (mostly cardiac surgery) and only ~15% from the ED
Patients got a median of 2L (1L -3.5L) of the study fluid, that’s it. These were not large volume resuscitations.
90% of patients received fluids prior to enrollment, 60% got balanced crystalloid and only 30% 0.9% NaCl.
HEAT– We can’t help treating fever. We like the numbers euboxic, elevated temp? It must be bad! Doctors, parents, nurses treat fever reflexively. Yet, there’s a thought that fever may be evolutionary and could potentially be protective. Treating pain or discomfort? That’s one thing, but here the authors sought to determine if there was a clinically important benefit to treating the number in ICU patients.
Randomised controlled, double blinded study of n=690 ICU patients with T>38F + suspected infection randomized to receive either 1 g paracetamol (acetaminophen/APAP) or placebo every 6 hours.
Primary outcome: median ICU-free days to day 28 – no difference 23 (IQR 13-25) in paracetamol group vs 22 in placebo group (IQR 12-25); P=0.07
No difference in secondary outcomes of mortality at 28 and 90 days
Limitations: ~30% of patients in both arms received open label APAP after the course of the study drug
Bottom Line Pearls:
It appears we may be SPLITting hairs over fluid choices. Giving a couple of liters? Fluid choice may not matter. SPLIT does not provide literature for larger volume resuscitations.
Treating fever in ICU patients with suspected infection doesn’t have an effect on ICU free days. Treat discomfort and pain with APAP but don’t expect to save lives or ICU beds by doing so.
“Negative studies” are important. So is examining our practice.
Jane Brody wrote an article, “What Comes After the Heimlich Maneuver” that ran in the NY Times and stirred up a ruckus on Twitter. This is a reasonable article on choking and details the limitations of the Heimlich maneuver. Unfortunately, the article ends instructing the layperson do to a cricothyrotomy (cric) with a sharp knife and “something like a straw or casing of a ballpoint pen (first remove the ink cartridge). “
Dr. Seth Trueger (@MDaware) wrote a post, Bad Idea Jeans, discouraging this practice saying that deciding which patient needs a cric is one of the more difficult but more important parts of this procedure.
On another note, our friend Dr. Andy Neill has found that medical students are able to perform crics with Papermate pens on cadavers [1]. However, it appears that most pens may not be suitable [2]. Further, while medical students are nearly lay people, we do not think this the cric should be within the domain of lay people (especially without patients already declared dead and preserved).
Cricothyrotomies – In reality, this is a bloody procedures that should only be done by those with proper training when the airway cannot be otherwise secured. The actual procedure has been detailed by those far smarter and with more experience than the FOAMcast crew. We recommend checking out Dr. Scott Weingart’s compilation of resources here.
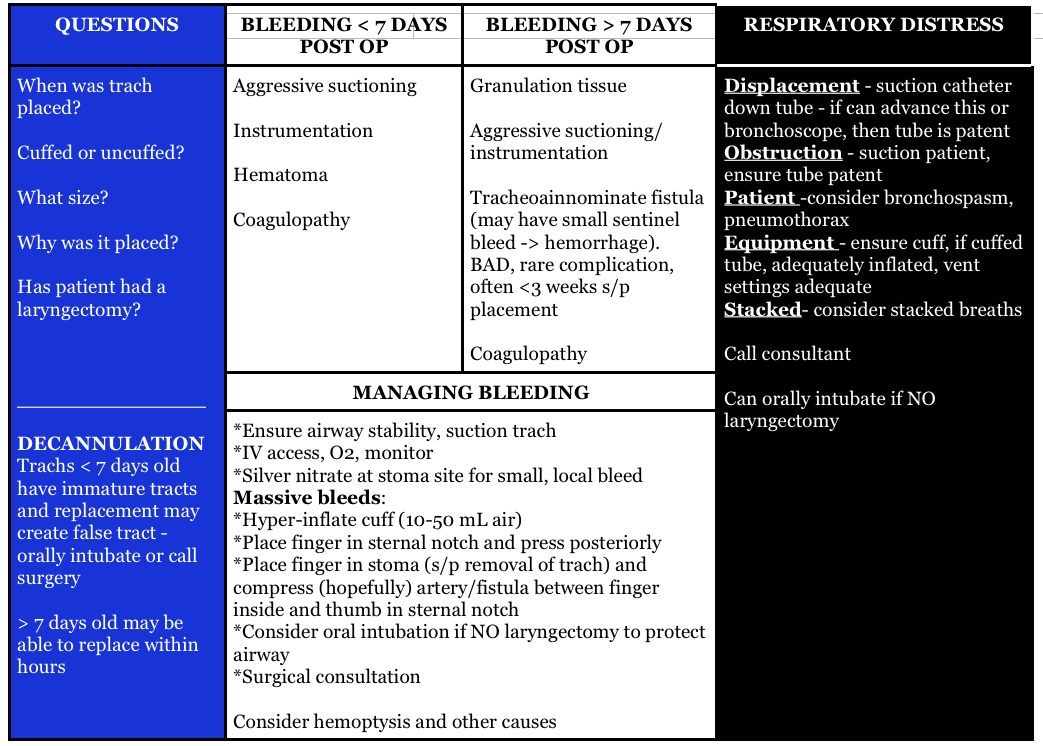
Question 1. A 72-year-old man who is 1 week out from an ischemic stroke presents with respiratory distress. He had a tracheostomy placed 6 days ago for sudden respiratory failure. The patient is hypoxic and tachypneic on presentation with minimal breath sounds bilaterally. There is no subcutaneous air around the stoma.[polldaddy poll=9110296]
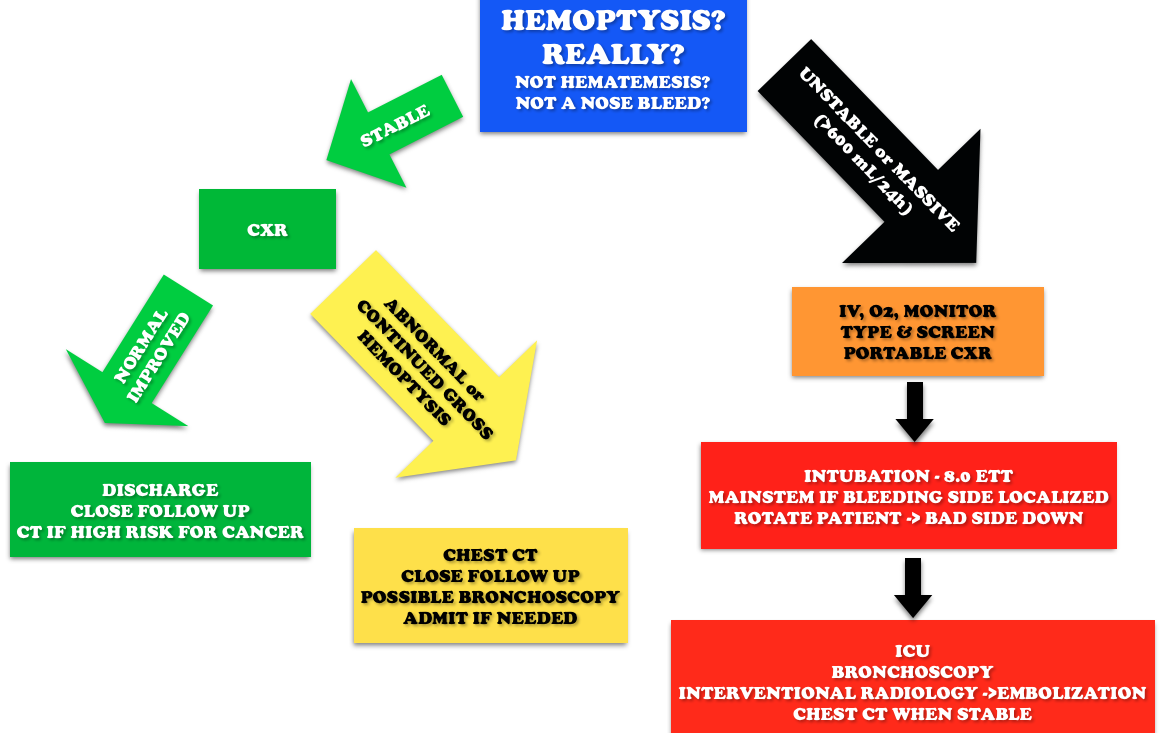
Question 2. A 3-year-old boy presents in severe respiratory distress. His mother informs you that he has been ill for the last 5 days, initially with a low-grade fever and “barky cough.” He was seen at an urgent care facility 4 days ago and given a “breathing treatment” and discharged on steroids. He has become progressively worse despite compliance with the steroid regimen, which prompted his mother to call an ambulance this morning. He is otherwise healthy and up-to-date on his immunizations. On examination, the child is toxic in appearance and febrile. His oropharynx is clear. You hear both inspiratory and expiratory stridor. [polldaddy poll=9110301]
Answers
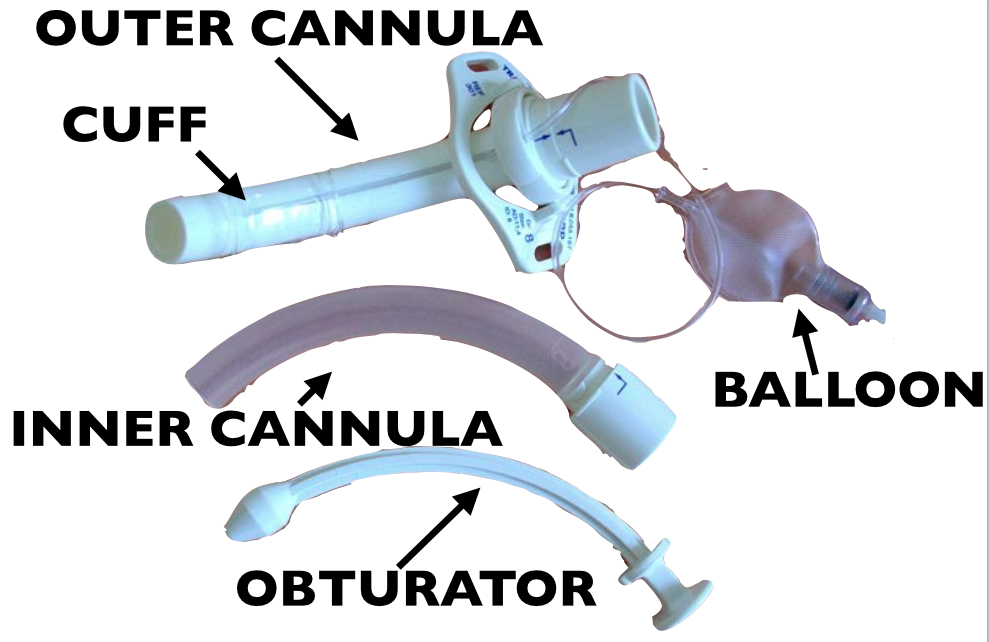
1.The patient’s presentation is concerning for airway obstruction and the first step in management is suctioning of the tracheostomy tube. Tracheostomy tubes are placed for long-term mechanical ventilation in patients with anticipated prolonged or permanent respiratory failure. The two most common complications are obstruction and dislodgement. Sudden onset of respiratory failure often indicates mucous plugging or equipment failure. Suctioning of the tracheostomy is a simple procedure that may quickly relieve the patient’s symptoms. 2 to 3 ml of normal saline should be instilled into the tube followed by suctioning. Patients with slower decline in respiratory status may have a worsening of their underlying pulmonary pathology or may have developed a pulmonary infection. A cricothyrotomy (A) will not lead to effective oxygenation or ventilation as the cricothyroid membrane is above the tracheostomy site. The tracheostomy tube should not be removed and replaced with either an endotracheal tube (C) or a new tracheostomy tube (B) at this time because the tracheostomy tract has not matured at 6 days (this usually occurs at 15-30 days). If equipment failure in the form of a tracheostomy tube malfunction is suspected, the tube should be replaced with fiberoptic visualization to ensure that a false lumen isn’t created.
2.The patient is suffering from acute bacterial tracheitis. Bacterial tracheitis is the result of severe inflammation of the epithelial lining of the trachea leading to thick mucopurulent secretion production. This clinically manifests as viral prodrome with fever, URI symptoms, barky cough and stridor that intensifies and progresses to include a toxic appearing child with signs of airway obstruction, inspiratory and expiratory stridor, cyanosis, and severe respiratory distress. Another clue is that the child has been treated with medications (aerosolized epinephrine and steroids) for croup and has not improved clinically. Bacterial tracheitis is most common in children between the ages of 3 to 5 years. Most patients require orotracheal intubation for respiratory distress and ICU admission. The patient should be started on broad-spectrum intravenous antibiotics. Croup (B) is the most common cause of upper airway distress and obstruction in children between 6 months to 6 years of age with peak incidence at 2 years of age. Croup begins as a prodrome of low-grade fever and URI symptoms and is characterized by a barky cough, inspiratory stridor, and hoarse voice. Children are less toxic in appearance and rarely develop respiratory failure. The mainstays of treatment are steroids and aerosolized epinephrine. Epiglottitis (C) is characterized by abrupt onset of fever and sore throat and children classically present with difficulty in breathing, anxiety, stridor and drooling. This is less common in vaccinated children, such as the patient above and typically occurs in slightly older children. There is generally not a prodrome associated with epiglottitis. Peritonsillar abscess (D) occurs more commonly during adolescence and presents with trismus, unilateral sore throat, fever, tonsillar asymmetry, and uvula deviation away from the affected tonsil. The age of this patient and normal oropharynx examination make this diagnosis very unlikely.
References:
Neill A, Anderson P. Observational cadaveric study of emergency bystander cricothyroidotomy with a ballpoint pen by untrained junior doctors and medical students. Emergency medicine journal : EMJ. 30(4):308-11. 2013. [pubmed]
Owens D, Greenwood B, Galley A, Tomkinson A, Woolley S. Airflow efficacy of ballpoint pen tubes: a consideration for use in bystander cricothyrotomy. Emergency medicine journal : EMJ. 27(4):317-20. 2010. [pubmed]
The blog Brown Coat Nation (University of Illinois, Chicago) has a new series entitled “Inconceivable.” The idea is to expose medical terminology that we tend to use incorrectly. The first installment is focused on the misuse of the term “left shift,” and it’s the focus of this FOAMcastini.
The Core Content
The correct use of the term “left shift” refers to the presence of banded (immature) neutrophils in the blood. It does not refer to an elevated white blood cell count with a high percentage of neutrophils. An elevated white blood cell count with an abnormally high percentage of neutrophils should be called “neutrophillic leukocytosis.” Only the presence of immature neutrophils in the periphery (including bands) can accurately be called a “left shift.”
The term “left shift” is derived from the diagrams of the six stages of neutrophil development in the bone marrow. On the far left, you see the most basic precursor: the myeloblast. On the far right of the diagram one finds the mature segmented neutrophil (also known as the “polymorphonuclear leukocyte, or PMN). But just to the left of that is the “banded” neutrophil (the 5th stage of neutrophil development in which the large band of nuclear material has not yet “disbanded” into segments).
When an infection runs rampant, sometimes the bone marrow runs out of mature neutrophils to send to the periphery. So, the marrow panics and releases immature banded neutrophils that normally would not be considered “ready for prime time.”
Here’s some relevant spaced repetition on SIRS: Along with leukocytosis (>12,000) and leukopenia (<4,000), Bandemia >10% is one of the SIRS criteria (Systemic Inflammatory Response Syndrome). Temperature (>38C or <36C), Heart rate >90 (“sirs-ycardia”), tachypnea (RR>20) or PCO2 <32) are the other SIRS criteria. The presence of at least two these categories constitutes “positive SIRS”. In pediatrics, the temperature, heart rate, and respiratory rates should be age-adjusted.
Check out our previous episode on appendicitis for a reminder on whether leukocytosis (with or without neutrophillic predominance) is useful in risk stratification.
The St. Emlyn’s team ran a post on the REVERT trial, which added a new spin to the traditional (and traditionally ineffective) Valsalva maneuver for stable supraventricular tachycardia (SVT). In this post, Dr. Rick Body goes through the trial covering not only the results but also drops pearls on methodology.
Randomized 433 patients with SVT to one of the following:
“Modified” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec and then placed supine with passive leg raise immediately after procedure (see video)
“Standard” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec while maintaining upright position
43% of the patients in modified Valsalva group versus 17% in the standard technique achieved sinus rhythm at one minute yielding an absolute risk reduction of 26.2% (p<0.001) with a number needed to treat of about 4 (3.8).
Core Content – Supraventricular Tachycardia (SVT) and Ventricular Tachycardia (VT)
Tintinalli (7e) Chapter 22; Rosen’s Emergency Medicine (8e) Chapter 79
SVT
Broad term referring to tachycardias originating above the ventricles, including the regular rhythms of sinus tachycardia, AV nodal reentrant tachycardia, AV reentrant tachycardia, and the irregular rhythms of multifocal atrial tachycardia, atrial fibrillation, and some forms of atrial flutter.
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients-
Valsalva maneuver – we like this method of having a patient blow on a syringe. Unfortunately, prior to the REVERT trial, the valsalva maneuver success rate has been documented ~19% [3].
Adenosine (0.1mg/kg or 6 mg in adult; 2nd dose 0.2 mg/kg or 12 mg in adult, with occasional dose adjustments) – administration can be tricky because of the drug’s short half life, necessitating proximal administration, elevation of the arm, and a quick saline flush afterwards. You can combine the adenosine IN the flush as detailed in this post, meaning no stopcock.
Calcium channel blockers or beta-blockers (verapamil, diltiazem or even metoprolol, esmolol) – Recently the calcium channel blockers have increased in popularity in the FOAM world and these are Rosenalli approved [4,5].
Diagnosis: Typically wide QRS complex (95% with QRS >120 ms) and fast (150-200 beats per minute).
SVT with abberency can have a wide complex but this should be treated as VT [4,5] (see this video)
Monomorphic – complexes have same morphology
Polymorphic – complexes of various morphologies, associated with poor prognosis [4,5]
Treatment:
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients with monomorphic VT–
Electrical cardioversion
Procainamide – Level B recommendation for first line treatment of monomorphic VT[6].
Amiodarone – common in the US but per the AHA guidelines “reasonable in patients with sustained monomorphic VT that is hemodynamically unstable, refractory to conversion with countershock, or recurrent despite procainamide or other agents. (Level of Evidence: C)” [6].
Note: Dangerous if prolonged QT [6]
Lidocaine – “may be reasonable” [6]
Stable patients with polymorphic VT –
Electrical cardioversion
Beta-blockers (particularly if ischemic)
Amiodarone
Cardiac catheterization if potentially ischemic cause [6]
Torsades de Pointes – withdraw offending agent, magnesium sulfate IV if “a few episodes” per the AHA
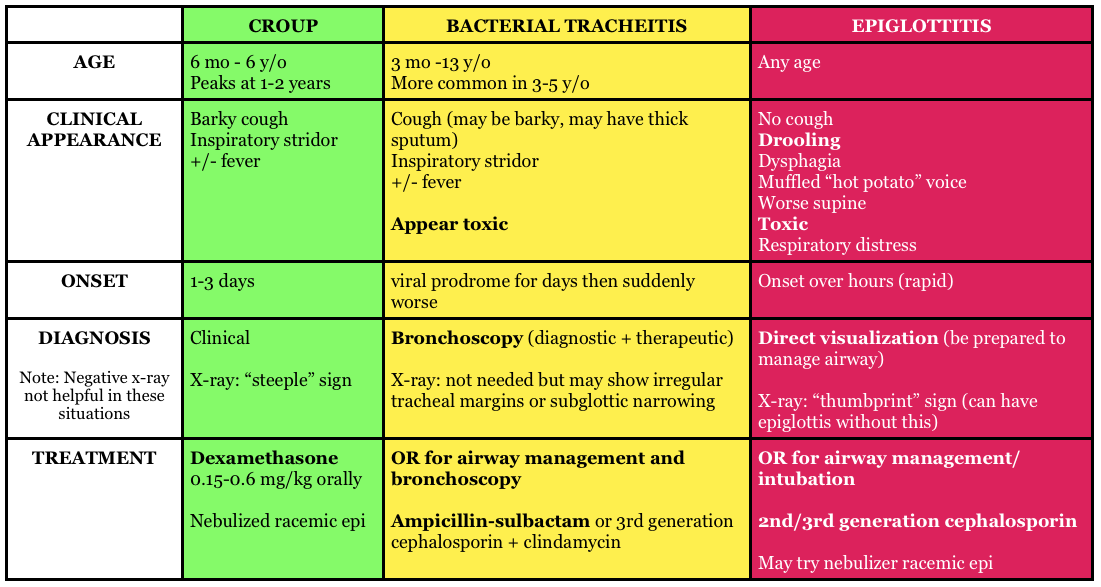
Question 1.A 26-year-old woman presents with dizziness and palpitations. She reports episodes of these symptoms beginning about 1 week ago, which initially only lasted a few minutes. However, for the past two days, she has had about 4 episodes a day which last about 20 minutes each. Her social history is significant for heavy caffeine intake. Her pulse is 166 bpm and her blood pressure is 140/70. Her rhythm strip is seen below. [polldaddy poll=9061960]
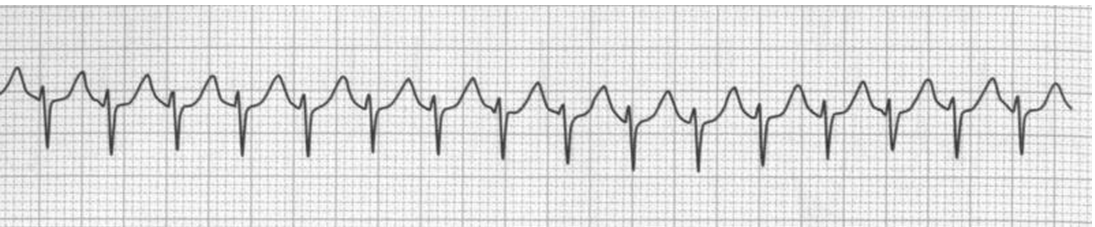
Question 2. A 33-year-old woman with chronic persistent asthma presents with palpitations. Her vital signs are HR 210, BP 118/73, and pulse oxygenation of 97% on room air. An ECG is shown below. [polldaddy poll=9061966]
Smith et al. Effectiveness of the Valsalva Manoeuvre for reversion of supraventricular tachycardia. Cochrane Database Syst Rev. 2013 Mar 28;3:CD009502. doi: 10.1002/14651858.CD009502.pub2
”Cardiac Rhythm Disturbances.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. pp 136-146.
The St. Emlyn’s team ran a post on the REVERT trial, which added a new spin to the traditional (and traditionally ineffective) Valsalva maneuver for stable supraventricular tachycardia (SVT). In this post, Dr. Rick Body goes through the trial covering not only the results but also drops pearls on methodology.
Randomized 433 patients with SVT to one of the following:
“Modified” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec and then placed supine with passive leg raise immediately after procedure (see video)
“Standard” Valsalva maneuver: patient sitting up performs Valsalva using a syringe to maintain 40 mm Hg for 15 sec while maintaining upright position
43% of the patients in modified Valsalva group versus 17% in the standard technique achieved sinus rhythm at one minute yielding an absolute risk reduction of 26.2% (p<0.001) with a number needed to treat of about 4 (3.8).
Core Content – Supraventricular Tachycardia (SVT) and Ventricular Tachycardia (VT)
Tintinalli (7e) Chapter 22; Rosen’s Emergency Medicine (8e) Chapter 79
SVT
Broad term referring to tachycardias originating above the ventricles, including the regular rhythms of sinus tachycardia, AV nodal reentrant tachycardia, AV reentrant tachycardia, and the irregular rhythms of multifocal atrial tachycardia, atrial fibrillation, and some forms of atrial flutter.
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients-
Valsalva maneuver – we like this method of having a patient blow on a syringe. Unfortunately, prior to the REVERT trial, the valsalva maneuver success rate has been documented ~19% [3].
Adenosine (0.1mg/kg or 6 mg in adult; 2nd dose 0.2 mg/kg or 12 mg in adult, with occasional dose adjustments) – administration can be tricky because of the drug’s short half life, necessitating proximal administration, elevation of the arm, and a quick saline flush afterwards. You can combine the adenosine IN the flush as detailed in this post, meaning no stopcock.
Calcium channel blockers or beta-blockers (verapamil, diltiazem or even metoprolol, esmolol) – Recently the calcium channel blockers have increased in popularity in the FOAM world and these are Rosenalli approved [4,5].
Diagnosis: Typically wide QRS complex (95% with QRS >120 ms) and fast (150-200 beats per minute).
SVT with abberency can have a wide complex but this should be treated as VT [4,5] (see this video)
Monomorphic – complexes have same morphology
Polymorphic – complexes of various morphologies, associated with poor prognosis [4,5]
Treatment:
Unstable patients – electrical cardioversion at 0.5-1 J/kg (100J for an adult) + ABCs!
Stable patients with monomorphic VT–
Electrical cardioversion
Procainamide – Level B recommendation for first line treatment of monomorphic VT[6].
Amiodarone – common in the US but per the AHA guidelines “reasonable in patients with sustained monomorphic VT that is hemodynamically unstable, refractory to conversion with countershock, or recurrent despite procainamide or other agents. (Level of Evidence: C)” [6].
Note: Dangerous if prolonged QT [6]
Lidocaine – “may be reasonable” [6]
Stable patients with polymorphic VT –
Electrical cardioversion
Beta-blockers (particularly if ischemic)
Amiodarone
Cardiac catheterization if potentially ischemic cause [6]
Torsades de Pointes – withdraw offending agent, magnesium sulfate IV if “a few episodes” per the AHA
Question 1.A 26-year-old woman presents with dizziness and palpitations. She reports episodes of these symptoms beginning about 1 week ago, which initially only lasted a few minutes. However, for the past two days, she has had about 4 episodes a day which last about 20 minutes each. Her social history is significant for heavy caffeine intake. Her pulse is 166 bpm and her blood pressure is 140/70. Her rhythm strip is seen below. [polldaddy poll=9061960]
Question 2. A 33-year-old woman with chronic persistent asthma presents with palpitations. Her vital signs are HR 210, BP 118/73, and pulse oxygenation of 97% on room air. An ECG is shown below. [polldaddy poll=9061966]
Smith et al. Effectiveness of the Valsalva Manoeuvre for reversion of supraventricular tachycardia. Cochrane Database Syst Rev. 2013 Mar 28;3:CD009502. doi: 10.1002/14651858.CD009502.pub2
”Cardiac Rhythm Disturbances.” Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. pp 136-146.
The paper: The authors took blood samples from 760 healthy pregnant patients at one point during their pregnancy. They propose a continuous increase for a normal d-dimer cut off throughout gestation.
1-12 weeks: n=33, 81% with normal d-dimer
19-21 weeks: n=53, 32% with normal d-dimer
28-36 weeks: n=8, 6% with normal d-dimer
39-40 weeks: 0, 0% normal d-dimer
Postpartum day 2: n=12, 8% with normal d-dimer
Dr. Radecki’s “Take Home:“
Dr. Kline has advocated for the following d-dimer cut offs in pregnancy: 1st trimester 750 ng/mL, 2nd trimester 1000 ng/mL, and 3rd trimester 1250 ng/mL(based on a standard cut-off of 500 ng/mL) and this may be reasonable but is not rooted in robust evidence.
Interestingly, this post was followed by another post covering an article by Hutchinson et al from Am J Roentgenol showing that of 174 CTPAs initially read as positive, 45 were read as negative by chest radiologist upon blinded retrospective review. That means 25.9% of this cohort diagnosed with PE apparently had negative CT scans.
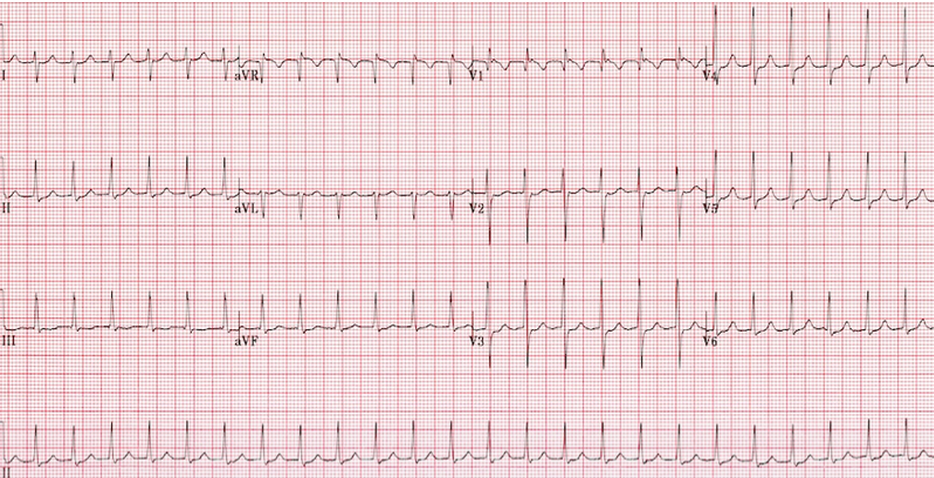
Core Content – Hemoptysis
Tintinalli (7e) Chapter 66; Rosen’s Emergency Medicine (8e) Chapter 24
Etiology: Most common causes are bronchitis (often blood tinged sputum), infection (abscess, pneumonia, tuberculosis), neoplasm (lung cancer). Other causes include iatrogenic causes (bronchoscopy, biopsy, aspirated foreign body), anticoagulation, and autoimmune diseases such as granulomatous polyangiitis (Wegener’s), lupus, and Goodpasture’s.
Question 1. A 50-year-old man, nonsmoker, presents to the ED with a 2-day history of cough now associated with frank hemoptysis. He denies any constitutional symptoms. Vital signs are BP 125/70, HR 80, RR 16, and pulse oximetry is 98% on room air. On exam, his lung fields are clear; the remainder of the exam is unremarkable. A chest radiograph is performed, which is normal. [polldaddy poll=9039260]
Question 2. A 55-year-old man, smoker, presents to the ED with hemoptysis and dyspnea for 4 weeks. His VS are T 37°C, BP 146/76 mm Hg, HR 85 bpm, RR 20 per minute, and oxygen saturation 96% on RA. His lung exam reveals distant breath sounds on the left side. His chest X-ray is shown below. [polldaddy poll=9039262]
Rosh Review
Answers
1.C. The patient is hemodynamically stable with a normal chest radiograph, so he does not require ICU admission (A). Patients with massive hemoptysis require ICU admission. The decision to perform a bronchoscopy (B) in this patient will be left up to the pulmonologist. Given the overall clinical picture, urgent bronchoscopy is not required in this case. With massive hemoptysis, an emergent bronchoscopy is indicated. Bronchitis (D) typically presents with the abrupt onset of cough with blood-streaked purulent sputum. The patient in the clinical scenario has persistent frank hemoptysis, which mandates further investigation. In a patient who does not smoke, is under the age of 40, and has a normal chest radiograph and scant hemoptysis, treatment for bronchitis can be initiated with outpatient follow-up.
2. B. Although bronchitis (A) is the most common cause of hemoptysis (responsible for 15%-30% of cases), patients present with cough as the dominant symptom and have abnormal lung exams and normal chest x-rays. The cough may be productive of sputum. The diagnosis of pneumonia (C) requires focal findings on physical exam or infiltrates on radiographic imaging and is typically accompanied by a fever. Patients with lung cancer are at increased risk for pulmonary embolism (D). This patient’s Wells score is 2 (one point each for hemoptysis and malignancy), which makes the likelihood of PE 16% in an ED population. Given the lung mass seen on chest x-ray, lung cancer is more likely than PE.
This week we cover a post from Dr. Rory Spiegel, author of EMnerd, on initial nonoperative management of acute appendicitis based on an article by Salminen et al in JAMA 2015.
530 patients with CT confirmed acute, uncomplicated appendicitis were randomized to operative intervention (n=273 receiving open laparotomies) or non-operative intervention (n=257 receiving antibiotics).
27.3% (n=70, CI 22-33.2%) of patients who received medical management (ertapenem x 3 days then 5 days of levofloxacin) had an appendectomy by the 1 year mark
7 patients (2.7%) in medical management group had complicated appendicitis at one year, 0 had abscesses
45 patients (20.5%) in the operative group had surgical complications
This is a non-inferiority study where the intent is to demonstrate that an experimental treatment (antibiotics alone) is not substantially worse than a control treatment (immediate surgery). The authors set the non-inferiority margin at 24%, which means that a failure rate (appendectomy by 1 year) >24% would render medical management inferior.
Authors Conclusion: “Among patients with CT-proven, uncomplicated appendicitis, antibiotic treatment did not meet the prespecified criterion for noninferiority compared with appendectomy.”
Spiegel’s Conclusion: “there is a great deal to be determined before this non-invasive strategy can be considered mainstream practice…in what was once considered an exclusively surgical disease, the majority of patients can effectively be managed conservatively. Despite not meeting their own high standards for non-inferiority, the authors demonstrated that for most patients with acute appendicitis, when treated conservatively with antibiotics we can avoid surgical intervention without complications of delays to definitive care.”
More FOAM on non-operative treatment of appendicitis: The SGEM
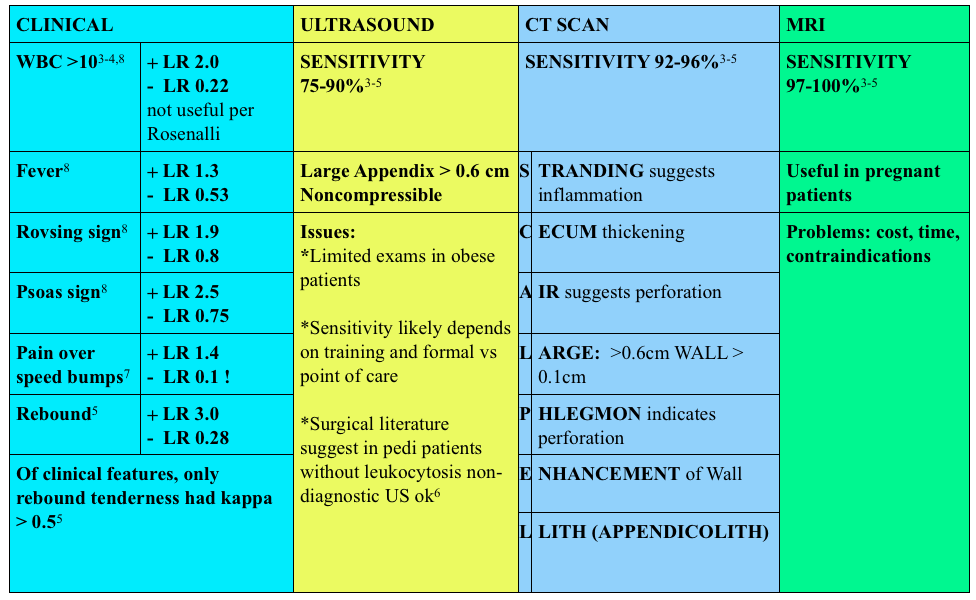
Use of contrast enhanced CT scans controversial. Rosenalli and the American College of radiology concur that oral contrast is probably not needed but does increase the emergency department length of stay [3-5].
Treatment:
Surgical consult
Antibiotics:
Broad spectrum beta-lactams: ampicillin-sulbactam 3g IV (75 mg/kg IV in peds) piperacillin-tazobactam 4.5g IV, cefoxitin 2g IV (40 mg/kg IV in peds) OR metronidazole 500 mg IV + ciprofloxacin 400 mg IV
Other things to consider in special populations in right lower quadrant:
1. A 22-year-old man presents with abdominal pain followed by vomiting for 1 day. His examination is significant for right lower quadrant tenderness to palpation. He has a negative Rovsing sign. [polldaddy poll=9026936]
2. A 22-year-old woman presents with lower abdominal pain and vaginal discharge. She is sexually active with men with inconsistent barrier protection. Her vitals are normal other than temperature of 101°F. On examination, there is yellow cervical discharge, no cervical motion tenderness, but uterine and left adnexal tenderness. An ultrasound does not show any evidence of tubo-ovarian abscess. [polldaddy poll=9026939]
Answers.
1. B. Sensitivity or the true positive rate measures the proportion of actual positives that are correctly identified as such. It is determined by dividing the number of true positives of the test by the number of true positives + false negatives. Tests with a high sensitivity are good for ruling out disease as the test has very few false negatives. A test with high sensitivity is advantageous as a screening tool as it misses very few people with the disease. The onset of pain before vomiting has been found to be as high as 100% sensitive in diagnosing acute appendicitis.Rovsing’s sign (D) (indirect tenderness) describes pain felt in the right lower quadrant upon palpation of the left lower quadrant. This sign signifies the presence of peritoneal irritation and has a sensitivity of 58%. Right lower quadrant pain (C) has a sensitivity of 81% and fever (A) has a sensitivity of 67%.
2.This patient presents with signs and symptoms consistent with pelvic inflammatory disease (PID) and should be treated with ceftriaxone 250 mg IM and 2 weeks of doxycycline. PID is an ascending infection beginning in the cervix and vagina and ascending to the upper genital tract. Neisseria gonorrhoeae and Chlamydia trachomatis are most commonly implicated. It can present with a myriad of symptoms although lower abdominal pain is the most common. Other symptoms include fever, cervical or vaginal discharge and dyspareunia. Pelvic examination reveals cervical motion tenderness (CMT), adnexal tenderness and vaginal or cervical discharge. Inadequately treated PID can lead to tubo-ovarian abscess, chronic dyspareunia and infertility. Due to the variable presentation and serious sequelae, the CDC recommends empiric treatment of all sexually active women who present with pelvic or abdominal pain and have any one of the following: 1) CMT, 2) adnexal tenderness or 3) uterine tenderness. Treatment should cover the most common organisms and typically consists of a third generation cephalosporin (ceftriaxone) and a prolonged course of doxycycline. Patients with systemic manifestations or difficulty tolerating PO should be admitted for management.Ceftriaxone and azithromycin (A) are used in the treatment of cervicitis or urethritis. Clindamycin (C) and metronidazole (D) are used in the treatment of bacterial vaginosis. References:
1.Salminen P, Paajanen H, Rautio T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015;313(23):2340
{kind=link}