FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. Weekend review, Day 1 review.
Scientific Assembly Day 2 Pearls
(there’s too much to choose from, so follow #ACEP14)
Simple Complaints in Patients with HIV – Dr. John Perkins
HIV is a risk factor for coronary artery disease (CAD) and these patients are prone to thrombotic complications [Boccara et al]
Dr. Amal Mattu has really championed this point, as in this videocast
Resuscitation Pearls – Dr. Scott Weingart
REBOA and ECMO are exciting and coming…but most of us don’t have them. Watch the literature.
“Normal” vital signs shouldn’t reassure us in trauma. Don’t wait for patients to become hypotensive (this is a danger of euboxia)
The Shock Index (Heart Rate/Systolic Blood Pressure) is one way to help detect badness amongst “normal” vital signs in these patients (See this post)
ACLS algorithms, they’re helpful for people who don’t specialize in resuscitation. Think about the individual patient and target interventions accordingly. Oh, and do good CPR.
The AHA supports this, for example, they recommend against the routine use of calcium and sodium bicarbonate [2010 Guidelines].
End of Life/Palliative Care – Dr. James Adams
Hospice and palliative care are INTENSIVE. Listen to Dr. Ashley Shreves on the EMCrit podcast if you’re not convinced of this (actually, listen regardless, it’s worth it).
A Do Not Resuscitate (DNR) order only speaks to whether or not a patient wants CPR if they die. No more, no less. But, for more on this, check out this blog post.
In general, physicians don’t broach end-of-life topics with patients. Dr. Adams quoted a statistic “Approximately 50% of doctors don’t know their patient’s resuscitation wishes.” The consensus in the room was that it really doesn’t take that much time to initiate these conversations but brief questions asking about a patient’s wishes, checking in to see if they have sufficient resources, or. (Lauren’s take on the topic).
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. Yesterday’s episode covered the council meetings.
Scientific Assembly Day 1 Pearls
Opening Session by Freakonomics hosts Steven Levitt and Stephen Dubner. Weird choice? It turns out that economists and physicians have a lot in common. What’s that? Probabilities. As physicians we like to think of ourselves as diagnosticians, but we’re more like probalisticians. We make predictions, hopefully based on the best evidence, our clinical expertise, and our patient’s values. People don’t remember the little stuff, like extra testing but they do tend to remember the more outlandish things, like the “amazing saves” or awful “misses.”
See this post by Dr. Simon Carley, in which he describes the ways in which physicians are really playing the odds and gambling.
Cardiology Pearls from Dr. Slovis.
Post cardiac arrest – targeted temperature management to 35-36 Celsius is the new 33 Celsius [Nielsen].
Many patients should probably go to the cath lab after arrest, but it’s still not clear exactly who benefits the most. STEMIs should probably go to the cath lab and, perhaps, non-STEMI ventricular fibrillation/tachycardia arrests. Apparently, 10-30% of these are actually STEMIs “on the inside” [More skeptical takes on this from Dr. Radecki here and here]
Infectious Disease Pearls from Dr. David Pigott – When someone returns from a developing nation, say, West Africa, the cause of their fever is not necessarily ebola. It’s probably an unknown, regular virus. It’s probably not ebola but it may be malaria which is quite common.
His thoughts on predictors of badness: Symptoms typically appear within 8-10 days although the “watch” period is 21 days. If a patient is in their second week of symptoms and are hemodynamically stable, then the patient has a pretty good shot.
Tox Pearls from Dr. Tim Erickson
Calcium channel blocker toxicity – you can try fluids, calcium, atropine, and vasopressors. For sick patients, however, insulin is the best bet (Note, FOAM is ahead of the curve: post on the lack of utility in glucagon from 2012).
Insulin bolus of 1 unit/kg followed by a drip of 1 unit/kg/h. Add dextrose at about 0.5 mg/kg/h, depending on their glucose.
Check glucose and potassium every 30 minutes, with the goal to keep the potassium 2.8-3.2, per Goldfrank.
Cyanide toxicity (discussed here) – if you’re thinking about it, please do NOT wait on a cyanide level, or any labs. Treat, with the current recommendation of intravenous hydroxocobalamin. There’s some discussion on the use of intramuscular cobinamide, which would be great in situations without IVs; however, this is largely untested in humans presently [Bebarta et al].
Dr. Scott Weingart – Catch the CO2 Wave (podcast). End tidal CO2 (ETCO2) – ETCO2 has become essential in monitoring patients in the ED. With anything we monitor, we really need to understand what we’re looking at as well as the interventions.
ETCO2 does NOT = PaCO2.
In most patients, the PaCO2 will be ~3-5 mmHg higher than their ETCO2.
This is because ETCO2 is really a measure of: PaCO2 (or production) but also cardiac output and alveolar ventilation. Thus, the ETCO2 may be falsely low in a patient with significant dead space, such as COPD, or with impaired cardiac output (heart failure).
FOAMcast is bringing you pearls from conferences we attend and, first up, the American College of Emergency Physicians annual meeting, ACEP14. However, Jeremy and I both worked overnights so we got into town a little late. Our friends and ACEP luminaries, Drs. Justin Hensley, Howie Mell, and Todd Slesinger.
Naloxone (Narcan) – The council approved resolutions in support of naloxone for everyone. There was also a resolution on developing a clinical policy for emergency physicians prescriptions of naloxone. Watch out for it.
Medical Marijuana – Apparently http://www.mindanews.com/buy-inderal/ every year brings some bickering about medical marijuana….and every year, the council defeats the resolutions. This year was no different…no support for medical marijuana from ACEP.
Emergency Department Pharmacists – These folks are indispensable in the ED (and in the FOAM world), and ACEP recognized this with the passing of Resolution 44 (what this means, clinically, not sure). And if you haven’t work with them – you’re missing out. We’re huge fans of EMPharmD and, naturally, Bryan Hayes (@PharmERToxGuy)
There’s also a lot of politics that goes into these bills, for that part, we got Dr. Kevin Klauer, Council Speaker on FOAMcast to explain.
But the real news… Dr. Kevin Klauer’s haircut.
Dr. Kevin Klauer’s former look
Wow, Klauer got a haircut. Amazing. Still the same brain, just no bangs flip… pic.twitter.com/hmYtKKQyHc
We review Dr. Scott Weingart’s episode 133 on pre-hospital REBOA (resuscitative endovascular balloon occlusion of the aorta). Weingart interviews Dr. Gareth Davies about the encounter, underscoring the increasing use of REBOA.
For a quick REBOA refresher, check out Episode 121.
REBOA (Review of REBOA) – First described in 1954 in the Korean War, this is a form of hemorrhage control below the level of the chest without having to do a thoracotomy with aortic cross clamping, which has sparse mortality benefit and can be dangerous to providers. Most of the REBOA literature is from swine models and case-series, although there are currently larger trials underway.
Outline of procedure – Obtain arterial access through the common femoral artery, pass a vascular sheath, float a balloon catheter to the appropriate section of the aorta, and inflate the balloon to occlude blood flow. The aorta is divided into three zones so that balloon occlusion is performed in Zone 1 for abdominal injuries or Zone 3 for pelvic injuries, while Zone 2 is a proposed no-occlusion zone.
The Bread and Butter
Rosen’s Chapter 46, 134 and Tintinalli Chapter 260.
Answer: More than most appreciate. The spleen filters the blood, removing abnormal or old red blood cells (RBCs), debris, and antibody coated bacteria from the bloodstream. It also serves as a reservoir for RBCs and platelets and synthesizes antibodies, opsonins, etc.
Diagnosis – suspect spleen trauma clinically, with hypotension, left upper quadrant abdominal pain, or even minimal trauma, especially after infectious mononucleosis.
CT with IV contrast (hemodynamically stable patients). While FAST and DPL can detect peritoneal free fluid, they can’t detect subcapsular bleeds.
Unstable patients – operating room versus interventional radiology
Grading – 1 is 1 (<1 cm laceration depth), 3 is 3 (>3 cm laceration depth). Everything else is somewhere in between. Higher grades typically result in more aggressive interventions. Historically these get operative intervention
Grade 1: < 1 cm laceration depth or<10% subcapsular hematoma
Grade 2: 1-3 cm laceration or 10-50% subcapsular
Grade 3: > 3 cm laceration depth or >50% subcapsular hematoma
Grade 3 or higher should be considered for angiography with embolization (Level II, III – EAST)
Grade 4: partially devascularized spleen or contrast blush
Grade 5: a very battered, devascularized spleen
There’s slightly more to spleen grading, check out this post from Dr. McGonigal
Trivia: The punctate extravasation sometimes seen on angiogram after blunt trauma?
Answer: The Seurat Spleen (pubmed), named after the pointillist painter.
Treatment –
Unstable patients: Operating room or Angiographic Intervention (IR) (Level II – EAST)
Note: Board exam? Send the patient to the OR. In reality, there is some practice variation. Many would still argue the patient belongs in the OR, some places have combined OR/IR suites, and some opt for IR.
Post splenectomy patients will need immunizations for the encapsulated bacteria
Stable patients: Nonoperative management, which often comprises in-hospital monitoring, serial abdominal exams and hematocrits, etc is becoming increasingly common as first line for higher grade splenic injuries. The key here is that the team must be able to take the patient to the OR or IR should the situation change. Angioembolization has also gained momentum as management
Benefits: Preserved immune function of the spleen/patient may get to keep their spleen (Banerjee et al)
Post-Splenectomy Sepsis (Review)– Most common in the first years after splenectomy and in children.
Presentation – Patients may present with a vague flu-like illness or gastroenteritis but may go on to develop septic shock, DIC, and multiorgan dysfunction. In addition, meningitis without overwhelming infection or shock is a common presentation of pneumococcal infection in asplenic patients.
Etiology – encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenza, and Neisseria meningitidis), capnocytophaga canimorsus (dog bites), and parasites such as babesiosis (endemic in New England), malaria, and ehrlichiosis.
Question 2. A 23-year-old man presents with a stab wound to the abdomen. His vital signs are HR 132, BP 88/45. He has a positive FAST.[polldaddy poll=8376283]
References:
Chapter 46, 134. Rosen’s Emergency Medicine, 8e.
Chapter 260. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
Answers.
1. C. Splenic artery aneurysms are the most common type of visceral arterial aneurysms, accounting for up to 60% of cases. Etiologies include arterial fibrodysplasia, portal hypertension, and increased splenic AV shunting in pregnancy. Clinical presentation is vague with left upper quadrant pain with radiation to the left shoulder or subscapular area. Most of the aneurysms are <2 cm in diameter; only 2% result in life-threatening rupture. Treatment is surgical resection if the patient is symptomatic. Otherwise, asymptomatic patients can undergo transcatheter embolization. Of those aneurysms that rupture, up to 95% occur in young pregnant women.
Hepatic artery aneurysms (A) represents 20% of visceral artery aneurysms and are caused by atherosclerosis, infection, and abdominal trauma. Clinical presentation can mimic cholecystitis. Inferior mesenteric artery aneurysms(B) are uncommon. Superior mesenteric artery aneurysms (D) are the 3rd-most common visceral aneurysms. IV drug abusers are at increased risk.
2. D. This patient presents with hemorrhagic shock from a penetrating abdominal trauma and should be immediately transferred to the operating room for an exploratory laparotomy. Stab wounds are the most common form of penetrating trauma. About 70% of anterior stab wounds penetrate the peritoneum. It is difficult to predict the specific organ injured based on the external location of the wound. Initial management should focus on securing the airway, assessing and supporting the patients breathing and circulation. IV access and supplemental oxygen should be provided. In hypotensive trauma patients, early blood transfusion should be initiated and consideration should be made for massive transfusion protocol. Concomitant with the primary and secondary survey, a Focused Assessment with Sonography for Trauma (FAST) exam should be performed. The speed and accuracy of the FAST has almost completely replaced the need for diagnostic peritoneal lavage. In a FAST exam, images are obtained of the splenorenal space, hepatorenal space (Morrison’s pouch), heart and bladder (pouch of Douglas). A FAST exam has high sensitivity in detecting as little as 100 ml of fluid. A FAST examination showing free fluid in any of the abdominal views in the presence of hypotension should lead to the patient being transported to the operating room for exploratory laparotomy according to the Advanced Trauma Life Support (ATLS) algorithm. Angiographic embolization (A) is useful in patients with pelvic fractures and bleeding from pelvic vessels. CT scan of the abdomen and pelvis (B) can be performed in trauma patients who are stable to further assess for injuries.Diagnostic peritoneal lavage (C) does not play a role in management of penetrating trauma patients with hypotension and positive FAST examination.
POUND- 4 criteria is very indicative of migraine (+LR 24), 3 criteria also likely (+LR 3), although most of this comes from the outpatient literature [1].
Pounding headache
hOurs: headache lasts 4-72 h without medication
Unilateral headaches
Nausea
Disabling: disrupts daily activities
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 159 ; Rosen’s 8(e) Chapter 20, 103 – but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
In Emergency Medicine, our job is to investigate and think about the life and limb threatening causes, even to mundane problems. Things such as intracranial bleeds, meningitis, masses – these are huge deals and are covered well and hammered into our heads. For FOAM core content on this, check out the St. Emlyn’s podcast. On this episode, we’re running a mini-ophthalmology headache special and focusing on headaches that treatment may render “sight saving.”
Temporal Arteritis – often in patients older than 50 years of age and more common in those with a history of polymyalgia rheumatica. May be accompanied by visual changes including the “classic” amaurosis fugax or “curtain” of unilateral vision loss. If not treated, these patient can lose vision permanently.
Unilateral or localized headache, often in the temporal or retro-orbital area
Jaw claudication (pain with chewing) – most specific sign
Decreased pulse in temporal artery or tenderness
Sedimentation Rate (ESR) >50
Treatment
Prednisone 40-60 mg if thinking about diagnosis
Temporal artery biopsy within 48 hrs
Acute Angle Closure Glaucoma– Classically, these patients present with unilateral mid-dilated pupils and severe nausea, vomiting, and headaches. The history can, naturally, be less classic and more vague. Also, if not treated, this can lead to vision loss.
They may want topical b-blocker, cholinergic, alpha-2 agonist, eye drops or administration of acetazolamide
Idiopathic Intracranial Hypertension(Pseudotumor Cerebri) – Common in young, overweight women or those on oral contraceptives. Untreated, they can suffer vision loss.
Elevated opening pressure (>20-25 cm H20) on lumbar puncture
Treatment
Neuro follow up
Acetazolamide +/- furosemide
Therapeutic lumbar punctures
Cerebral Venous Sinus Thrombosis – may present as atypical headache with stroke like symptoms in patients without known vascular risk factors. The neurological findings may be transient. Often associated with post-partum patients, patients with hypercoaguable states (Factor V mutations, protein C or S deficiency, antithrombin III deficiency, etc), patients on OCPs.
Diagnosis – CTV or MRV (magnetic resonance venography) after CT scan, which may be normal.
Treatment – Anticoagulation, although this is somewhat controversial
Question 1. A 73-year-old woman with a history of hypertension presents with a unilateral headache for 3 weeks. She states that she has a throbbing pain at her right temple and has pain in her jaw with opening and closing. The vision in her right eye has worsened over the previous day. Her blood pressure is 173/100.
[polldaddy poll=8340282]
Question 2. A 71-year-old woman presents to the ED with daily headaches for 2 months. She describes the headache as a dull pain that is most intense in the morning and resolves by the afternoon. On exam you note 4/5 motor weakness of the left upper and lower extremity.
3.Chapter 159. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
Answers
1. D. This patient presents with a unilateral, subacute headache with associated jaw claudication and vision change; symptoms consistent with temporal arteritis. Temporal arteritis or giant cell arteritis is a systemic inflammatory process of small and medium-size arteries. The most commonly involved vessels are the ophthalmic vessels and the extracranial branches of the aortic arch. The disease typically affects patients over 70 years of age and is more common in women than in men. Patients present with a subacute headache that is throbbing in nature and may be present for weeks to months. Often, patients will have symptoms for more than 2 months. Patients may also report jaw claudication secondary to vascular insufficiency of the masseter and temporalis muscles. Physical examination may reveal tenderness over the temporal artery. Systemic symptoms may also be present including fever, joint pains, and weight loss. Diagnostic testing in the Emergency Department generally begins with an erythrocyte sedimentation rate (ESR) with a cutoff of 50 mm/hour although the level may be >100 mm/hour. However, the ESR will be normal in 10-25% of patients. The gold standard diagnostic test is a temporal artery biopsy. In patients with a high-clinical likelihood of temporal arteritis, treatment should be initiated regardless of initial diagnostic testing as delay can lead to permanent visual loss. Prednisone should be started at 60 – 120 mg/day.
Carbamazepine (A) is the treatment of choice for trigeminal neuralgia, not temporal arteritis. The patient does not present with symptoms consistent with hypertensive emergency requiring emergent antihypertensive treatment withlabetalol (B). A non-contrast head CT scan (C) is not helpful in temporal arteritis as the disease does not involve the intracranial contents.
2. B More than half of patients diagnosed with a brain tumor complain of headache. However, the headache associated with brain tumor is highly variable. Patients may describe it as continuous or intermittent, unilateral or bilateral, sharp or dull. It is associated with neurologic deficits less than 10% of the time. However, in the setting of aneurologic deficit and chronic headache (as in this scenario with motor weakness), a mass lesion should be strongly considered as the cause. Patients may also complain of nausea, vomiting, visual change, and gait disturbance. Headaches due to brain tumors are classically associated with pain that is worse in the morning (as in this case). However, this is rare.
Central venous thrombosis (A) results from hypercoagulable states and is associated with acute to subacute headaches with vomiting and sometimes seizures. Risk factors include the use of oral contraceptives, postpartum or postoperative states, and any hypercoagulable state such as factor V Leiden mutation, antithrombin III deficiency, protein S or C deficiency, or polycythemia. The diagnosis is usually made by MRI venogram. Migraine headache (C) is classified as a primary headache and can be quite variable in presentation. These headaches can be associated with nausea, vomiting, photophobia, and phonophobia. The headache may also be preceded or accompanied by an aura that develops gradually over minutes, usually lasts 60 minutes, and is reversible. Auras may include neurologic symptom but commonly include scintillating scotomas (dark spots) or flashing lights. Temporal arteritis (D) occurs almost exclusively in patients older than 50 years and is much more common in women. Headache is the most common symptom of temporal arteritis and usually occurs over the frontotemporal region. It is strongly associated with a history of polymyalgia rheumatic. It is not associated with focal neurologic deficits, but it can lead to vision loss due to ischemic optic neuritis.
POUND- 4 criteria is very indicative of migraine (+LR 24), 3 criteria also likely (+LR 3), although most of this comes from the outpatient literature [1].
Pounding headache
hOurs: headache lasts 4-72 h without medication
Unilateral headaches
Nausea
Disabling: disrupts daily activities
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 159 ; Rosen’s 8(e) Chapter 20, 103 – but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
In Emergency Medicine, our job is to investigate and think about the life and limb threatening causes, even to mundane problems. Things such as intracranial bleeds, meningitis, masses – these are huge deals and are covered well and hammered into our heads. For FOAM core content on this, check out the St. Emlyn’s podcast. On this episode, we’re running a mini-ophthalmology headache special and focusing on headaches that treatment may render “sight saving.”
Temporal Arteritis – often in patients older than 50 years of age and more common in those with a history of polymyalgia rheumatica. May be accompanied by visual changes including the “classic” amaurosis fugax or “curtain” of unilateral vision loss. If not treated, these patient can lose vision permanently.
Unilateral or localized headache, often in the temporal or retro-orbital area
Jaw claudication (pain with chewing) – most specific sign
Decreased pulse in temporal artery or tenderness
Sedimentation Rate (ESR) >50
Treatment
Prednisone 40-60 mg if thinking about diagnosis
Temporal artery biopsy within 48 hrs
Acute Angle Closure Glaucoma– Classically, these patients present with unilateral mid-dilated pupils and severe nausea, vomiting, and headaches. The history can, naturally, be less classic and more vague. Also, if not treated, this can lead to vision loss.
They may want topical b-blocker, cholinergic, alpha-2 agonist, eye drops or administration of acetazolamide
Idiopathic Intracranial Hypertension(Pseudotumor Cerebri) – Common in young, overweight women or those on oral contraceptives. Untreated, they can suffer vision loss.
Elevated opening pressure (>20-25 cm H20) on lumbar puncture
Treatment
Neuro follow up
Acetazolamide +/- furosemide
Therapeutic lumbar punctures
Cerebral Venous Sinus Thrombosis – may present as atypical headache with stroke like symptoms in patients without known vascular risk factors. The neurological findings may be transient. Often associated with post-partum patients, patients with hypercoaguable states (Factor V mutations, protein C or S deficiency, antithrombin III deficiency, etc), patients on OCPs.
Diagnosis – CTV or MRV (magnetic resonance venography) after CT scan, which may be normal.
Treatment – Anticoagulation, although this is somewhat controversial
Question 1. A 73-year-old woman with a history of hypertension presents with a unilateral headache for 3 weeks. She states that she has a throbbing pain at her right temple and has pain in her jaw with opening and closing. The vision in her right eye has worsened over the previous day. Her blood pressure is 173/100.
[polldaddy poll=8340282]
Question 2. A 71-year-old woman presents to the ED with daily headaches for 2 months. She describes the headache as a dull pain that is most intense in the morning and resolves by the afternoon. On exam you note 4/5 motor weakness of the left upper and lower extremity.
3.Chapter 159. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
Answers
1. D. This patient presents with a unilateral, subacute headache with associated jaw claudication and vision change; symptoms consistent with temporal arteritis. Temporal arteritis or giant cell arteritis is a systemic inflammatory process of small and medium-size arteries. The most commonly involved vessels are the ophthalmic vessels and the extracranial branches of the aortic arch. The disease typically affects patients over 70 years of age and is more common in women than in men. Patients present with a subacute headache that is throbbing in nature and may be present for weeks to months. Often, patients will have symptoms for more than 2 months. Patients may also report jaw claudication secondary to vascular insufficiency of the masseter and temporalis muscles. Physical examination may reveal tenderness over the temporal artery. Systemic symptoms may also be present including fever, joint pains, and weight loss. Diagnostic testing in the Emergency Department generally begins with an erythrocyte sedimentation rate (ESR) with a cutoff of 50 mm/hour although the level may be >100 mm/hour. However, the ESR will be normal in 10-25% of patients. The gold standard diagnostic test is a temporal artery biopsy. In patients with a high-clinical likelihood of temporal arteritis, treatment should be initiated regardless of initial diagnostic testing as delay can lead to permanent visual loss. Prednisone should be started at 60 – 120 mg/day.
Carbamazepine (A) is the treatment of choice for trigeminal neuralgia, not temporal arteritis. The patient does not present with symptoms consistent with hypertensive emergency requiring emergent antihypertensive treatment withlabetalol (B). A non-contrast head CT scan (C) is not helpful in temporal arteritis as the disease does not involve the intracranial contents.
2. B More than half of patients diagnosed with a brain tumor complain of headache. However, the headache associated with brain tumor is highly variable. Patients may describe it as continuous or intermittent, unilateral or bilateral, sharp or dull. It is associated with neurologic deficits less than 10% of the time. However, in the setting of aneurologic deficit and chronic headache (as in this scenario with motor weakness), a mass lesion should be strongly considered as the cause. Patients may also complain of nausea, vomiting, visual change, and gait disturbance. Headaches due to brain tumors are classically associated with pain that is worse in the morning (as in this case). However, this is rare.
Central venous thrombosis (A) results from hypercoagulable states and is associated with acute to subacute headaches with vomiting and sometimes seizures. Risk factors include the use of oral contraceptives, postpartum or postoperative states, and any hypercoagulable state such as factor V Leiden mutation, antithrombin III deficiency, protein S or C deficiency, or polycythemia. The diagnosis is usually made by MRI venogram. Migraine headache (C) is classified as a primary headache and can be quite variable in presentation. These headaches can be associated with nausea, vomiting, photophobia, and phonophobia. The headache may also be preceded or accompanied by an aura that develops gradually over minutes, usually lasts 60 minutes, and is reversible. Auras may include neurologic symptom but commonly include scintillating scotomas (dark spots) or flashing lights. Temporal arteritis (D) occurs almost exclusively in patients older than 50 years and is much more common in women. Headache is the most common symptom of temporal arteritis and usually occurs over the frontotemporal region. It is strongly associated with a history of polymyalgia rheumatic. It is not associated with focal neurologic deficits, but it can lead to vision loss due to ischemic optic neuritis.
In this tiny episode, Jeremy reviews his favorite pearl from each episode, loooking at episodes 4-14. Why the repetition? Well, it turns out we learn better when information is spaced in small aliquots over time (spaced repetition).
Right Ventricle MI: ST elevation in lead III greater than lead II – you know what to do (cath lab). ST elevation in II greater than III – think pericarditee (pericarditis).
Right sided leads: elevation in V4R most specific but elevation in V3R-6R are indicative of RVMI.
Strong Ion Difference (SID), which is the difference between the sums of concentrations of the strong cations and strong ions (typically Sodium minus Chloride). Small SID = acidic (example SID of 0.9% NaCl = 0)
The discriminatory zone is out. Get ultrasounds in pregnant patients, regardless of the quantitative beta-hCG. A certain beta-hCG level can not be used to rule in or rule out ectopic pregnancy or viable intrauterine pregnancy (IUP), get the ultrasound and ensure you identify the uterus.
Biphasic anaphylaxis is extremely rare and prolonged ED observation does not really help as these reactions can occur up to 6 days later. Rosenalli recommend observation 2-4 hours.
No clear cut winner in the beta-blocker vs. calcium channel blocker battle
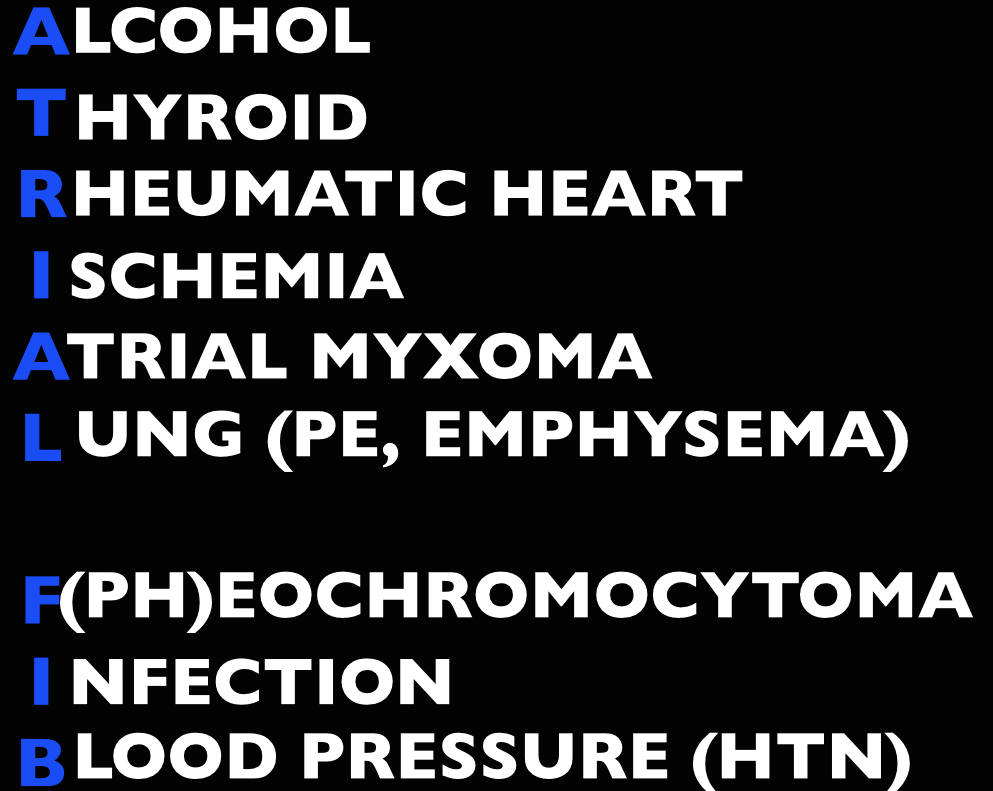
Long Term Atrial Fibrillation Management in General:
Avoid beta-blockers in:
Obstructive lung disease (asthma/COPD)
Peripheral vascular disease
Diabetics
Severe congestive heart failure (CHF)
Erectile dysfunction
Avoid calcium-channel blockers in:
Severe CHF and acute decompensated heart failure (ADHF)
Of note, in patients
The Maryland Critical Care Project has a great post with many of Dr. Amal Mattu’s key FOAM talks embedded on Tachydysrhythmias You Gotta Know.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 280, 295 ; Rosen’s 8(e) Chapter 50 – a well written chapter, but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Pads in either an anterior-lateral (AL) or anterior-posterior (AP) position followed by synchronized cardioversion at 100-200 J biphasic. Current literature shows no significant difference in pad placement [1]
Rate control. A target of <120 beats per minute is acceptable in the ED [2-3]. First line agents are nodal blocking agents such as diltiazem and metoprolol
Diltiazem 0.25 mg/kg IV over 2 minutes with a peak effect in 2-7 minutes. Can repeat at 0.35 mg/kg IV over 2 minutes.
Metoprolol 5-10 mg IV.
Rhythm control with cardioversion. While there’s no proven benefit to rhythm control, many patients would prefer to be in sinus rhythm and ED cardioversion of stable new-onset atrial fibrillation is appropriate in a select population, notably, when the onset is <48 hours (or <72 hours per Rosen). The pooled literature suggests a thromboembolism rate <0.8% [4].
Note: A recent article in JAMA by Nuotio et al found a higher rate of embolic events in patients who were electively cardioverted after >12 hours in atrial fibrillation.The 30 day risk of thromboembolism when cardioverted between 12-48 hours was 1.1%, compared to the ~2% risk if cardioverted after 48 hours. While the risk is still small, it is higher than the ~0.3% risk of thromboembolism with anticoagulation on board.
Treat the underlying cause (ex: sepsis, pulmonary embolism, hyperthyroidism, etc)
May also consider Amiodarone, Digoxin (mean >11 hours to rate control) [3]
In atrial fibrillation with pre-excitation (WPW), an often wide and irregular rhythm with different/changing morphologies to the QRS do NOT treat with an AV Nodal blocking agent as this may result in death (Adenosine, Beta-blocker, Calcium-channel blocker, etc). Treat with procainamide or shock
Disposition – Admit patients that present unstable, with underlying co-morbidities, or those that are not rate controlled. Depending on the patient’s follow up and local practice patterns, the
More sensitive to electrical cardioversion, less sensitive to chemical cardioversion
Multifocal Atrial Tachycardia
Irregular narrow complex tachycardia with p waves of at least 3 morphologies (this can be difficult to see, so look in multiple leads, particularly V2)
Etiology -often seen in advanced pulmonary disease
Management – Treat the underlying cause, do NOT cardiovert MAT
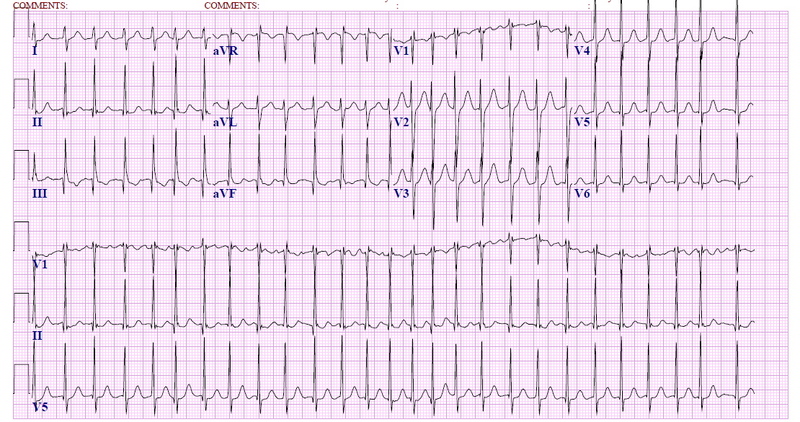
Question 1. A 72-year-old man with a history of hypertension, diabetes, and congestive heart failure presents to the ED with heart palpitations for the past 4 days. He denies any chest pain, shortness of breath, abdominal pain, or history of similar palpitations. In the ED, his vital signs are BP 135/75, HR 138, RR 14, and oxygen saturation 98% on room air. His ECG is seen below. Which of the following is the most appropriate next step in management?
Rosh Review
A. Chemical cardioversion
B. Rate Control
C. Synchronized cardioversion
D. Warfarin
Question 2. When do you worry about giving calcium channel blockers, beta-blockers, or digoxin in a patient with atrial fibrillation?
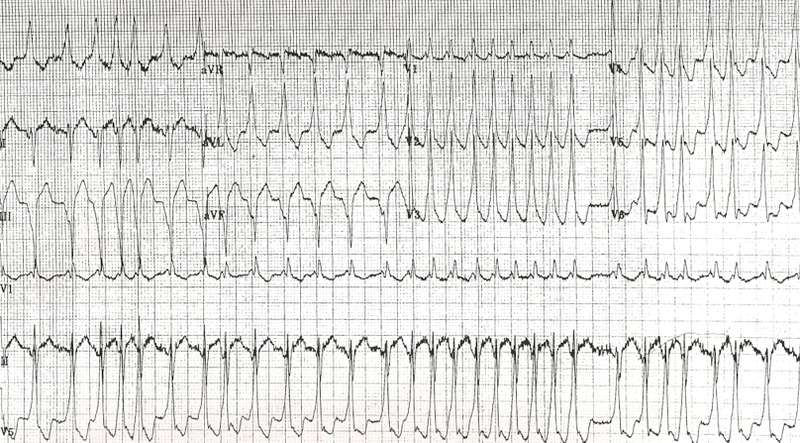
Question 3. An 18-year-old woman presents with palpitations and near syncope. Her vitals are T 98.7F, HR 199, BP 113/66, RR 32, and oxygen saturation 94%. Her ECG is shown below. What treatment is indicated?
Rosh Review
A. Administer adenosine 6 mg IV
B. Administer diltiazem 10 mg IV
C. Administer lopressor 10 mg IV
D. Administer procainamide 100mg IV
References
1. Kirkland S, Stiell I, AlShawabkeh T, Campbell S, Dickinson G, Rowe BH. The Efficacy of Pad Placement for Electrical Cardioversion of Atrial Fibrillation/Flutter: A Systematic Review. Acad Emerg Med. 2014;21(7):717–726.
2. Chapter. Rosen’s Emergency Medicine, 8e.
3.Chapter. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
4. Cohn BG, Keim SM, Yealy DM. Is Emergency Department Cardioversion of Recent-onset Atrial Fibrillation Safe and Effective? J Emerg Med. 2013;45(1):117–27.
Answers
1. B. Atrial fibrillation is caused by chaotic, disorderly firing from a second focus within the atria, resulting in uncoordinated atrial contractions. Patients with atrial fibrillation may present with palpitations, chest pain, shortness of breath, or they may be asymptomatic. Atrial fibrillation can be classified as chronic or paroxysmal, with paroxysms lasting minutes to days. On ECG, there are irregularly irregular narrow QRS complexes. In addition, no discernible p-waves are noted, rather fibrillatory waves are seen. Unless the patient is hemodynamically unstable, the mainstay of therapy is rate control. This is achieved through medications that act on the AV node such as calcium channel blockers (eg diltiazem or verapamil), beta-blockers, or digoxin. Due to digoxin’s slow onset of action and side effects, it is considered a second line medication.
If atrial fibrillation has been present for >48 hours, there is an increased risk of atrial thrombus formation. An echocardiogram should be obtained in these patients to exclude thrombus formation prior to rhythm control. Patients with chronic atrial fibrillation usually are placed on warfarin (D) or a similar anticoagulant to prevent thromboembolism.Chemical cardioversion (A) (amiorodone, procainamide or flecainide) can be attempted in patients with paroxysmal atrial fibrillation for less than 48 hours. Synchronized cardioversion (C) is used in patients who are hemodynamically unstable. This can be achieved by administering 50 – 100 J of electricity in synchronization mode.
2. If a patient has an accessory pathway, such as Wolff-Parkinson-White Syndrome.
3. D. This patient presents with near syncope in the setting of atrial fibrillation with abberant conduction most likely secondary to Wolff-Parkinson-White (WPW) syndrome and should be chemically or electrically cardioverted. WPW syndrome refers to the presence of an accessory pathway between the right atrium and right ventricle. This accessory pathway has a shortened refractory period and can bypass normal conduction down the AV node. Because of the shortened refractory time, the accessory pathway in WPW can conduct atrial impulses much faster than the AV node can allowing for a ventricular rate between 150 and 300 beats per minute. Any tachycardia greater than 200 beats per minute in an adult should raise suspicion for an accessory pathway.
Patients with WPW can be asymptomatic or may present with severe tachydysrhythmias. The most common presenting dysrhythmia is reentrant tachycardia (70-80%) and second is atrial fibrillation (10-30%). In these tachydysrhythmias, the patient can conduct orthodromically (down the AV node and back up the accessory pathway), antidromically (down the accessory pathway and up the AV node) or in both directions. Patients who have any antidromic conduction will present with wide complex tachycardias. In patients with irregularly irregular wide-complex tachycardias, atrial fibrillation with WPW is the most common diagnosis. If the patient is unstable, electrical cardioversion should be pursued immediately as these patients run the risk of degrading into ventricular tachycardia and ventricular fibrillation. If the patient is stable, procainamide can be administered for chemical cardioversion. Procainamide is a class Ia anitdysrhythmic agent. The dose of procainamide (D) is 18-20 mg/kg administered at a rate of 20-30 mg/min.
In patients with WPW, antidysrhythmic agents that block the AV node are contraindicated. Blocking the AV node causes unopposed electrical conduction down the accessory pathway. This can lead to ventricular dysrhythmias. Additionally, the accessory pathway in WPW responds paradoxically to AV nodal blocking agents by further decreasing its refractory time. Adenosine (A), beta-blockers (C), calcium-channel blockers (B) and digoxin all block the AV node.
No clear cut winner in the beta-blocker vs. calcium channel blocker battle
Long Term Atrial Fibrillation Management in General:
Avoid beta-blockers in:
Obstructive lung disease (asthma/COPD)
Peripheral vascular disease
Diabetics
Severe congestive heart failure (CHF)
Erectile dysfunction
Avoid calcium-channel blockers in:
Severe CHF and acute decompensated heart failure (ADHF)
Of note, in patients
The Maryland Critical Care Project has a great post with many of Dr. Amal Mattu’s key FOAM talks embedded on Tachydysrhythmias You Gotta Know.
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 280, 295 ; Rosen’s 8(e) Chapter 50 – a well written chapter, but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Pads in either an anterior-lateral (AL) or anterior-posterior (AP) position followed by synchronized cardioversion at 100-200 J biphasic. Current literature shows no significant difference in pad placement [1]
Rate control. A target of <120 beats per minute is acceptable in the ED [2-3]. First line agents are nodal blocking agents such as diltiazem and metoprolol
Diltiazem 0.25 mg/kg IV over 2 minutes with a peak effect in 2-7 minutes. Can repeat at 0.35 mg/kg IV over 2 minutes.
Metoprolol 5-10 mg IV.
Rhythm control with cardioversion. While there’s no proven benefit to rhythm control, many patients would prefer to be in sinus rhythm and ED cardioversion of stable new-onset atrial fibrillation is appropriate in a select population, notably, when the onset is <48 hours (or <72 hours per Rosen). The pooled literature suggests a thromboembolism rate <0.8% [4].
Note: A recent article in JAMA by Nuotio et al found a higher rate of embolic events in patients who were electively cardioverted after >12 hours in atrial fibrillation.The 30 day risk of thromboembolism when cardioverted between 12-48 hours was 1.1%, compared to the ~2% risk if cardioverted after 48 hours. While the risk is still small, it is higher than the ~0.3% risk of thromboembolism with anticoagulation on board.
Treat the underlying cause (ex: sepsis, pulmonary embolism, hyperthyroidism, etc)
May also consider Amiodarone, Digoxin (mean >11 hours to rate control) [3]
In atrial fibrillation with pre-excitation (WPW), an often wide and irregular rhythm with different/changing morphologies to the QRS do NOT treat with an AV Nodal blocking agent as this may result in death (Adenosine, Beta-blocker, Calcium-channel blocker, etc). Treat with procainamide or shock
Disposition – Admit patients that present unstable, with underlying co-morbidities, or those that are not rate controlled. Depending on the patient’s follow up and local practice patterns, the
More sensitive to electrical cardioversion, less sensitive to chemical cardioversion
Multifocal Atrial Tachycardia
Irregular narrow complex tachycardia with p waves of at least 3 morphologies (this can be difficult to see, so look in multiple leads, particularly V2)
Etiology -often seen in advanced pulmonary disease
Management – Treat the underlying cause, do NOT cardiovert MAT
Question 1. A 72-year-old man with a history of hypertension, diabetes, and congestive heart failure presents to the ED with heart palpitations for the past 4 days. He denies any chest pain, shortness of breath, abdominal pain, or history of similar palpitations. In the ED, his vital signs are BP 135/75, HR 138, RR 14, and oxygen saturation 98% on room air. His ECG is seen below. Which of the following is the most appropriate next step in management?
Rosh Review
A. Chemical cardioversion
B. Rate Control
C. Synchronized cardioversion
D. Warfarin
Question 2. When do you worry about giving calcium channel blockers, beta-blockers, or digoxin in a patient with atrial fibrillation?
Question 3. An 18-year-old woman presents with palpitations and near syncope. Her vitals are T 98.7F, HR 199, BP 113/66, RR 32, and oxygen saturation 94%. Her ECG is shown below. What treatment is indicated?
Rosh Review
A. Administer adenosine 6 mg IV
B. Administer diltiazem 10 mg IV
C. Administer lopressor 10 mg IV
D. Administer procainamide 100mg IV
References
1. Kirkland S, Stiell I, AlShawabkeh T, Campbell S, Dickinson G, Rowe BH. The Efficacy of Pad Placement for Electrical Cardioversion of Atrial Fibrillation/Flutter: A Systematic Review. Acad Emerg Med. 2014;21(7):717–726.
2. Chapter. Rosen’s Emergency Medicine, 8e.
3.Chapter. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
4. Cohn BG, Keim SM, Yealy DM. Is Emergency Department Cardioversion of Recent-onset Atrial Fibrillation Safe and Effective? J Emerg Med. 2013;45(1):117–27.
Answers
1. B. Atrial fibrillation is caused by chaotic, disorderly firing from a second focus within the atria, resulting in uncoordinated atrial contractions. Patients with atrial fibrillation may present with palpitations, chest pain, shortness of breath, or they may be asymptomatic. Atrial fibrillation can be classified as chronic or paroxysmal, with paroxysms lasting minutes to days. On ECG, there are irregularly irregular narrow QRS complexes. In addition, no discernible p-waves are noted, rather fibrillatory waves are seen. Unless the patient is hemodynamically unstable, the mainstay of therapy is rate control. This is achieved through medications that act on the AV node such as calcium channel blockers (eg diltiazem or verapamil), beta-blockers, or digoxin. Due to digoxin’s slow onset of action and side effects, it is considered a second line medication.
If atrial fibrillation has been present for >48 hours, there is an increased risk of atrial thrombus formation. An echocardiogram should be obtained in these patients to exclude thrombus formation prior to rhythm control. Patients with chronic atrial fibrillation usually are placed on warfarin (D) or a similar anticoagulant to prevent thromboembolism.Chemical cardioversion (A) (amiorodone, procainamide or flecainide) can be attempted in patients with paroxysmal atrial fibrillation for less than 48 hours. Synchronized cardioversion (C) is used in patients who are hemodynamically unstable. This can be achieved by administering 50 – 100 J of electricity in synchronization mode.
2. If a patient has an accessory pathway, such as Wolff-Parkinson-White Syndrome.
3. D. This patient presents with near syncope in the setting of atrial fibrillation with abberant conduction most likely secondary to Wolff-Parkinson-White (WPW) syndrome and should be chemically or electrically cardioverted. WPW syndrome refers to the presence of an accessory pathway between the right atrium and right ventricle. This accessory pathway has a shortened refractory period and can bypass normal conduction down the AV node. Because of the shortened refractory time, the accessory pathway in WPW can conduct atrial impulses much faster than the AV node can allowing for a ventricular rate between 150 and 300 beats per minute. Any tachycardia greater than 200 beats per minute in an adult should raise suspicion for an accessory pathway.
Patients with WPW can be asymptomatic or may present with severe tachydysrhythmias. The most common presenting dysrhythmia is reentrant tachycardia (70-80%) and second is atrial fibrillation (10-30%). In these tachydysrhythmias, the patient can conduct orthodromically (down the AV node and back up the accessory pathway), antidromically (down the accessory pathway and up the AV node) or in both directions. Patients who have any antidromic conduction will present with wide complex tachycardias. In patients with irregularly irregular wide-complex tachycardias, atrial fibrillation with WPW is the most common diagnosis. If the patient is unstable, electrical cardioversion should be pursued immediately as these patients run the risk of degrading into ventricular tachycardia and ventricular fibrillation. If the patient is stable, procainamide can be administered for chemical cardioversion. Procainamide is a class Ia anitdysrhythmic agent. The dose of procainamide (D) is 18-20 mg/kg administered at a rate of 20-30 mg/min.
In patients with WPW, antidysrhythmic agents that block the AV node are contraindicated. Blocking the AV node causes unopposed electrical conduction down the accessory pathway. This can lead to ventricular dysrhythmias. Additionally, the accessory pathway in WPW responds paradoxically to AV nodal blocking agents by further decreasing its refractory time. Adenosine (A), beta-blockers (C), calcium-channel blockers (B) and digoxin all block the AV node.
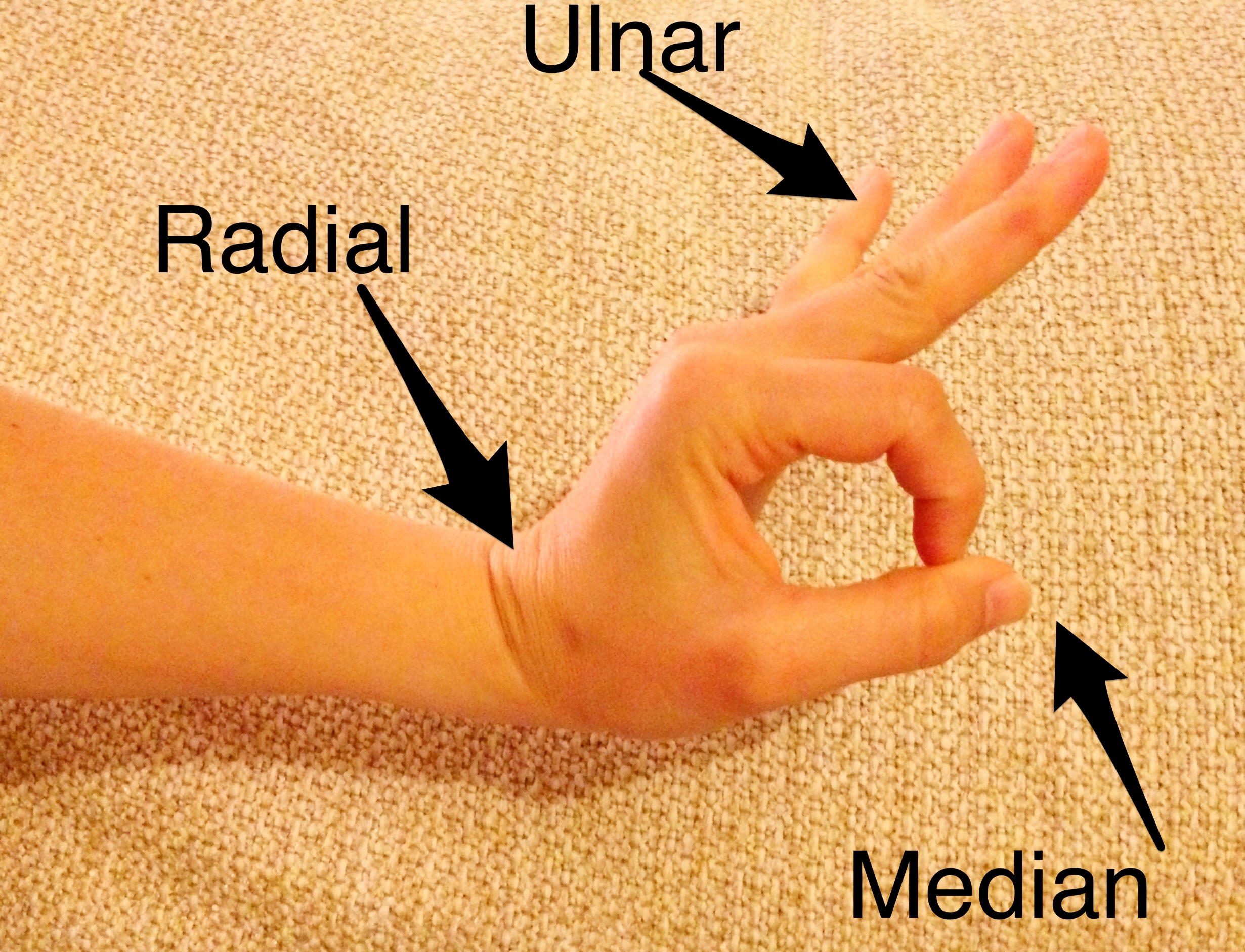
All 3 motor nerves (median, ulnar, radial) in one motion:
Make the “ok sign” and try to break the ring formed by the thumb and index finger – median
Memory aid: The median is “ok.”
Spread 3-5 fingers apart and adduct against resistance – ulnar
Memory aid: The intertriginous areas between abducted fingers make a “U” for ulnar
Dorsiflex wrist – radial
Memory aid…if you look really hard, the the dorsiflexed hand and arm appear to be a sideways, lower case “r”
…all in one
Motor Exam of the Hand
The Bread and Butter
We summarize some key topics from the following readings, Tintinalli (7e) Chapter 280, 295 ; Rosen’s 8(e) Chapter 50 – a well written chapter, but, the point isn’t to just take our word for it. Go enrich your fundamental understanding yourself!
Flexor Tenosynovitis
Kanavel’s Cardinal Signs (look for words that start with “F”).
Pain on passive extension -happens early
Finger held in flexion – see above point..extension hurts!
Fusiform (uniform) swelling of finger – most common
Tenderness along flexor tendon sheath – happens later [3]
Treatment – serious surgical emergency and failure to treat adequately can result in necrosis, proximal spread, and loss of use of hand.
Mallet Finger: Disruption of the distal extensor tendons, often caused by a jamming injury, hyperextension, or crush. Look for bruising at the distal interphalangeal joint. Closed injury – immobilization. Open- extensor tendon repair.
High pressure injection injuries (paint gun, on the job stuff): Worse than they look. Tetanus, IV antibiotics, consult hand.
Digit amputation storage: Cover the stump with saline gauze and wrap amputated digit in saline soaked gauze. Put the saline soaked gauze covered digit in airtight plastic bag and place that bag in a bag on ice.
Amputations have best success of reimplantation if they are:
Clean cut (saw, etc) versus a crush injury
Distal (distal finger > proximal finger > hand)
Learn to Splint Like a Pro (via ERCast) and document a thorough neurovascular exam pre and post-splinting.
Question 1. Which of the following is classically seen in flexor tenosynovitis?
A. Extended position of the involved digit
B. Fusiform swelling of the digit
C. Tenderness over the extensor sheath
D. Vesicular eruption over the flexor surface
Question 2. A 42-year-old man presents to the ED with an amputation of his left thumb just proximal to the interphalangeal joint. The injury occurred 1 hour ago at a rural construction site while the patient was operating a power miter saw. The thumb is brought in, in a sandwich bag, along with the patient. Which of the following is true regarding predictors of successful replantation?
A. Crush injuries have a high success rate of replantation
B. Digits have better tolerance for ischemia than limbs have
C. The amputated part should be kept cold and dry
D. The patient’s social history adds little value to the success rate of replantation
2.Chapters 40, 280, 295. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011
3. Draeger RW, Bynum DK Jr. Flexor tendon sheath infections of the hand. J Am Acad Orthop Surg. 2012 Jun;20(6):373-82. doi: 10.5435/JAAOS-20-06-373.
Answers.
1. B. The flexor tendons of the fingers are covered by a double layer of synovium to promote gliding of the tendon underneath. Infections in the synovial spaces in the hand tend to spread along the course of the flexor tendon sheaths and may extend proximally to the hand. Infections are usually due to penetrating trauma involving the sheath but occasionally from hematogenous spread. Four cardinal signs of acute flexor tenosynovitis are usually present to help distinguish tenosynovitis from other hand infections. These criteria are referred to as the Kanavel’s signs. Flexor tenosynovitis is a surgical emergency. Consultation with a hand surgeon is warranted along with intravenous antibiotics. The affected digit is held in a flexed (A), not extended, posture. The tenderness is over the flexor (C) sheath, not extensor. Vesicles (D) are not commonly associated with flexor tenosynovitis. A localized herpes simplex infection may cause vesicles to form on a digit
2. B. Ischemia time is one of the most important predictors of successful replantation. Digits have less muscle mass to oxygenate and tolerate ischemia better than amputations more proximally along the limb. Replantation of limbs must be completed within 4–6 hours, but digits can tolerate an ischemic time of up to 8 hours, given proper preservation. Crush injuries (A) have a low success rate for replantation due to the significant destruction of neurovascular structures. The amputated body part should be irrigated with normal saline to remove gross contamination, wrapped insterile gauze moistened with saline (C), and placed in a sterile, watertight container. This container should be placed in ice water, but the digit itself should not be submerged. Research has repeatedly shown that tobacco use (D), especially smoking after surgery, will worsen the chance of successful replantation. Obtaining a social history is important in these cases.