(ITUNES OR LISTEN HERE)
Sleep through 2015? We picked the minds of some brilliant Emergency Medicine folk and came up with this short list of important happenings.
TRAUMA
FAST (Focused Assessment using Sonography in Trauma) guided resuscitative – thoracotomy. (Recommended by Haney Mallemat, Rob Orman).
Bottom Line: If a trauma code comes in and has neither cardiac activity nor pericardial effusion on FAST, the odds of survival are essentially nil. Inaba and colleagues found the following:
- Population: 187 patients at LA/USC deemed “appropriate” for thoracotomy (at this institution: penetrating trauma patients with absent vital signs and blunt trauma patients with a loss of vital signs en route or in the resuscitation bay).
- Intervention: Emergency medicine resident performed FAST before/concurrent with thoracotomy
- Outcome: Of the 126 patients without cardiac activity on FAST, none survived.
Many of the patients with cardiac activity did not survive, as well. This paper gives individuals guidance to make the decision to crack the chest but has stirred up a debate as to whether this would lessen educational opportunities for a potentially heroic procedure.
Say NO to long backboards (Recommended by Lauren Westafer). In January 2015, ACEP recommended against the use of long backboards. Many state and local protocols shifted away from moving this some time ago and even more since. The FOAM community has been up in arms about the inefficacies and harms of backboards for quite some time, again echoing that FOAM can serve as a forecaster for change to make it less cognitively distressing when time to change our practice.
RESUSCITATION
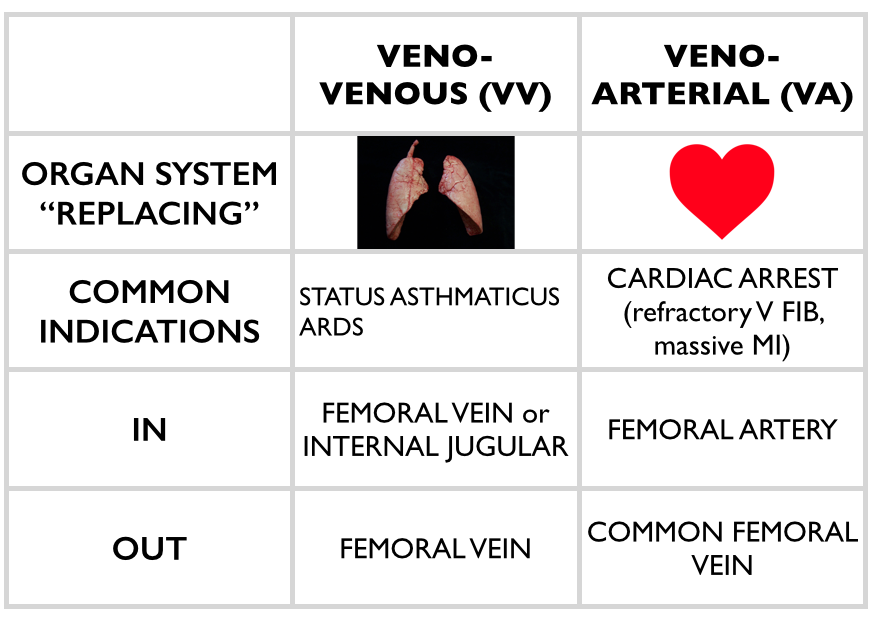
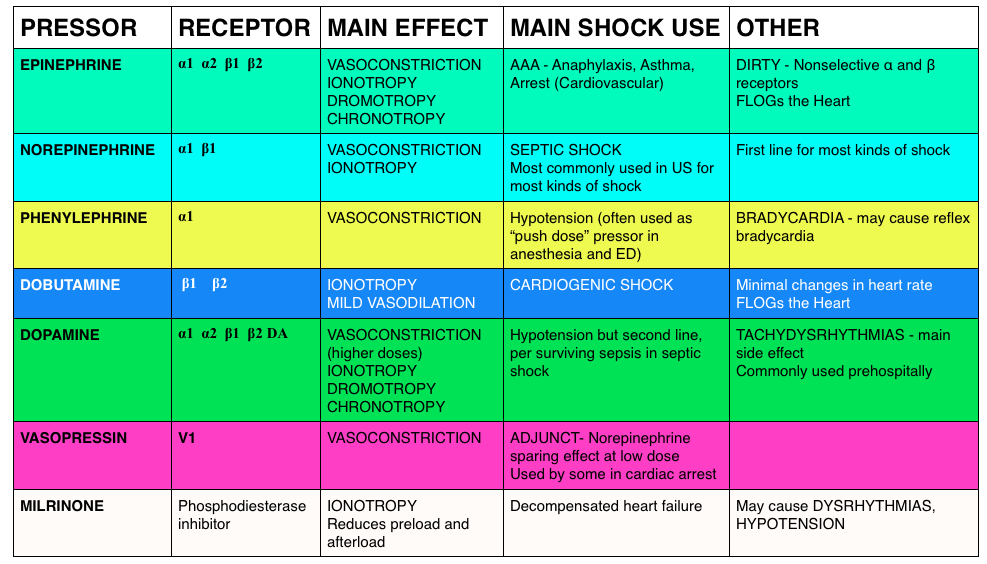
Peripheral Vasopressors (Recommended by Haney Mallemat, Rob Orman) – We detail the literature underlying the use of peripheral vasopressors in this podcast.
They think that the combination of a systematic review by Loubani et al and The Cardenas-Garcia study, peripheral vasopressors may be safely run through large bore peripheral IVs proximal to the antecubital fossa. Note: These should be closely monitored (protocolized is best) and short durations (<6 h) have been associated with minimal complicaitons.
SEPSIS
Intravenous fluids in sepsis (Recommended by Haney Mallemat). The PROMISE trial was published in early 2015, adding to ProCESS and ARISE. In these studies, patients typically got 2 L of crystalloid upfront and then 2L in the first 6 hours. Over 3 days after enrollment, most got just under 4 L. Most patients received under 6L IVF. There has been a movement for more judicious use of fluids in sepsis rather than dumping 4-6 L of IVF upfront. Marik articulately explained this in this article.
- Mallemat challenges us: Before giving a fluid bolus use ultrasound and ask these questions, “Does the LV need it, and can the RV take it?”
CMS Core Measure (Recommended by Jeremy Faust). The National Quality Forum has been pushing for Measure 0500 See this EMcrit podcast on this topic.
ANALGESIA
Pain control in acute low back pain is tricky, and opioids may not help (Recommended by David Newman).
RENAL
Sexual intercourse 3-4 times per week may aid in expulsion of distal kidney stones. This year, two large studies by Pickard et al and Furyk et al demonstrated no benefit in stone passage for ureterolithiasis (particularly in stones <5 mm). Then, a paper by Dolouglu et al excited many folks, if for entertainment value. Since tamsulosin doesn’t seem to help, what about sexual intercourse, 3-4 times per week, in male patients with partners?
In this study the mean expulsion time did not differ significantly between groups.
MEDICAL EDUCATION
Merging of FOAM resources. (Recommended by Michelle Lin). Blogs and podcasts are growing and often supplement one another. Dr. Lin predicts the future will be in these conglomerates (ex: merging of EMcrit and PulmCrit and massive undertakings such as ALiEM and CandiEM).
Merging of FOAM with traditional journals. (Recommended by Michelle Lin). Projects such as the Skeptic’s Guide to Emergency Medicine have merged with Academic Emergency Medicine and the Canadian Journal of Emergency Medicine (ex: SGEM HOP, journal paper) and massive FOAM resource ALiEM has also collaborated with Annals of Emergency Medicine (Ex:Journal club, paper). The merging of FOAM with paid, traditional resources is the future, per Dr. Lin.
OVERDIAGNOSIS
Overdiagnosis is a problem, and people are starting to rage against it. (Recommended by Lauren Westafer). An Overdiagnosis conference exists and JAMA Internal Medicine has a series of articles, “Less is More,” frequently detailing evidence of overdiagnosis.
- One of 2015’s prominent articles for emergency physicians was the Hutchinson et al study. In this study, CTPA scans read as positive for pulmonary embolism underwent review by 3 chest radiologist who adjudicated that, actually, 25.9% of the “positive” scans (n=45) did not actually have pulmonary embolisms. The harms from this exist beyond the risk of anticoagulation (think about how an ED approach for a myriad of complaints differs for a patient with a history of thromboembolism).
The FOAM community swelled with appreciation and respect for the late Dr. John Hinds. Please watch his SMACC talk, “Crack the Chest, Get Crucified,” in which his excellence in medical education shines, delivering pearls for nearly anyone.